Downloaded 418 times
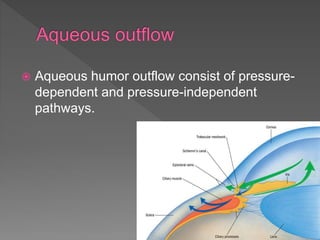
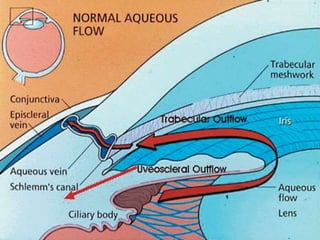






Aqueous humor is formed by the ciliary processes and flows from the posterior to anterior chamber, exiting through the trabecular and uveoscleral routes. It is continuously formed and drained at a rate of approximately 2.5mL/min. Aqueous outflow occurs through pressure-dependent (trabecular) and pressure-independent (uveoscleral) pathways. Various receptors and drugs that act on these pathways to regulate intraocular pressure are discussed. Common glaucoma medications include prostaglandin analogs, beta-blockers, alpha agonists, cholinergic agonists, and carbonic anhydrase inhibitors.














































































