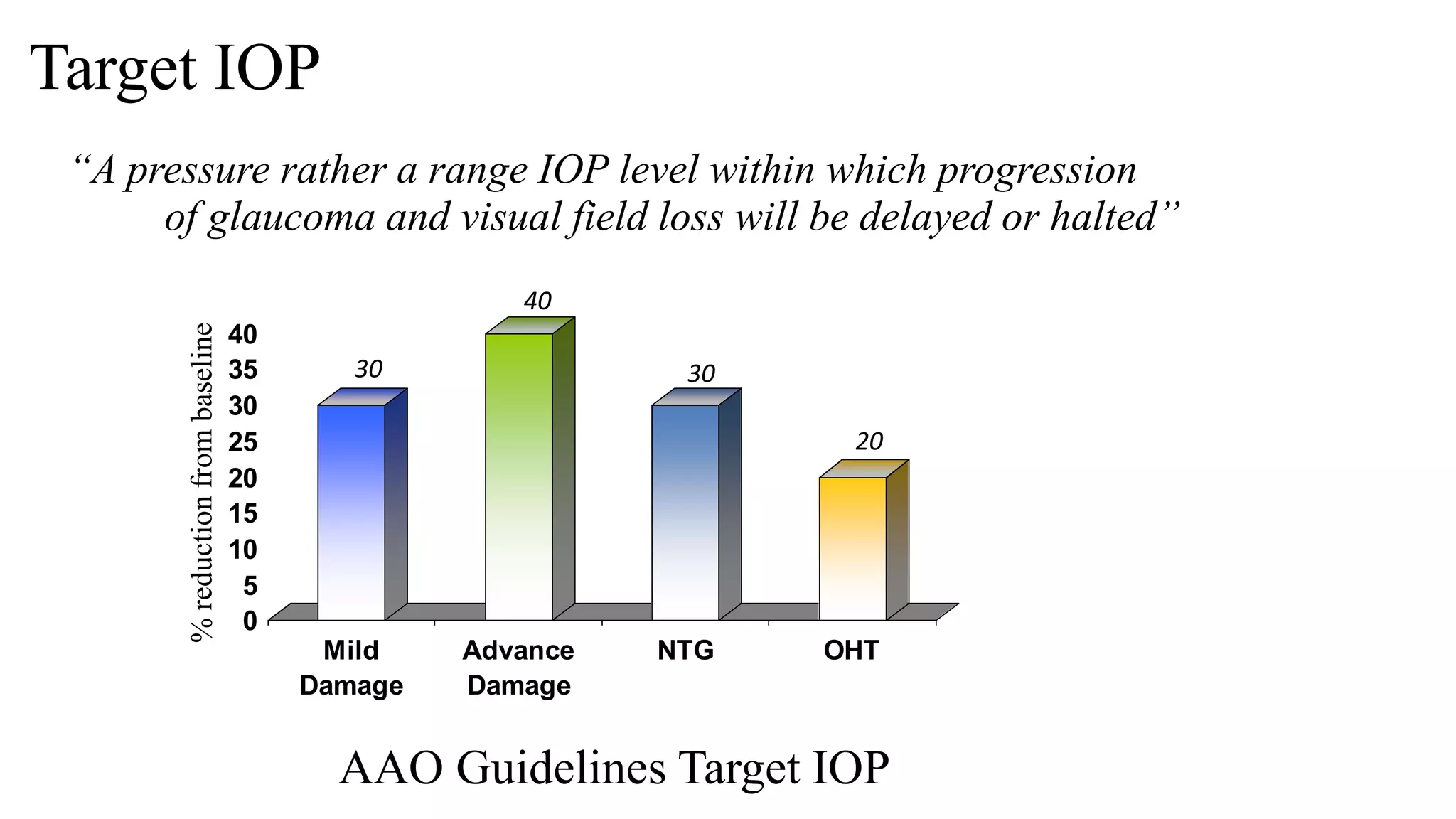
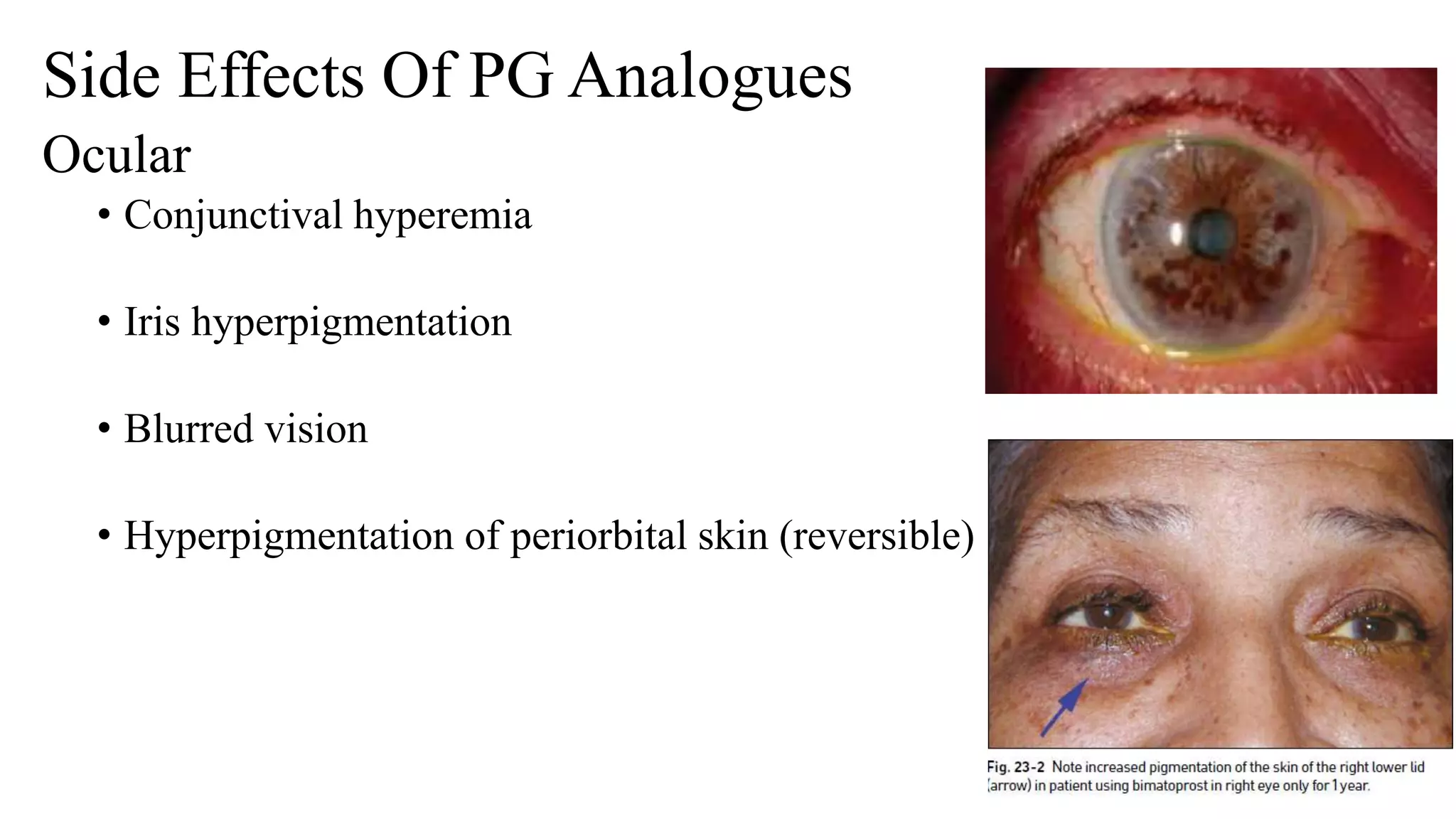
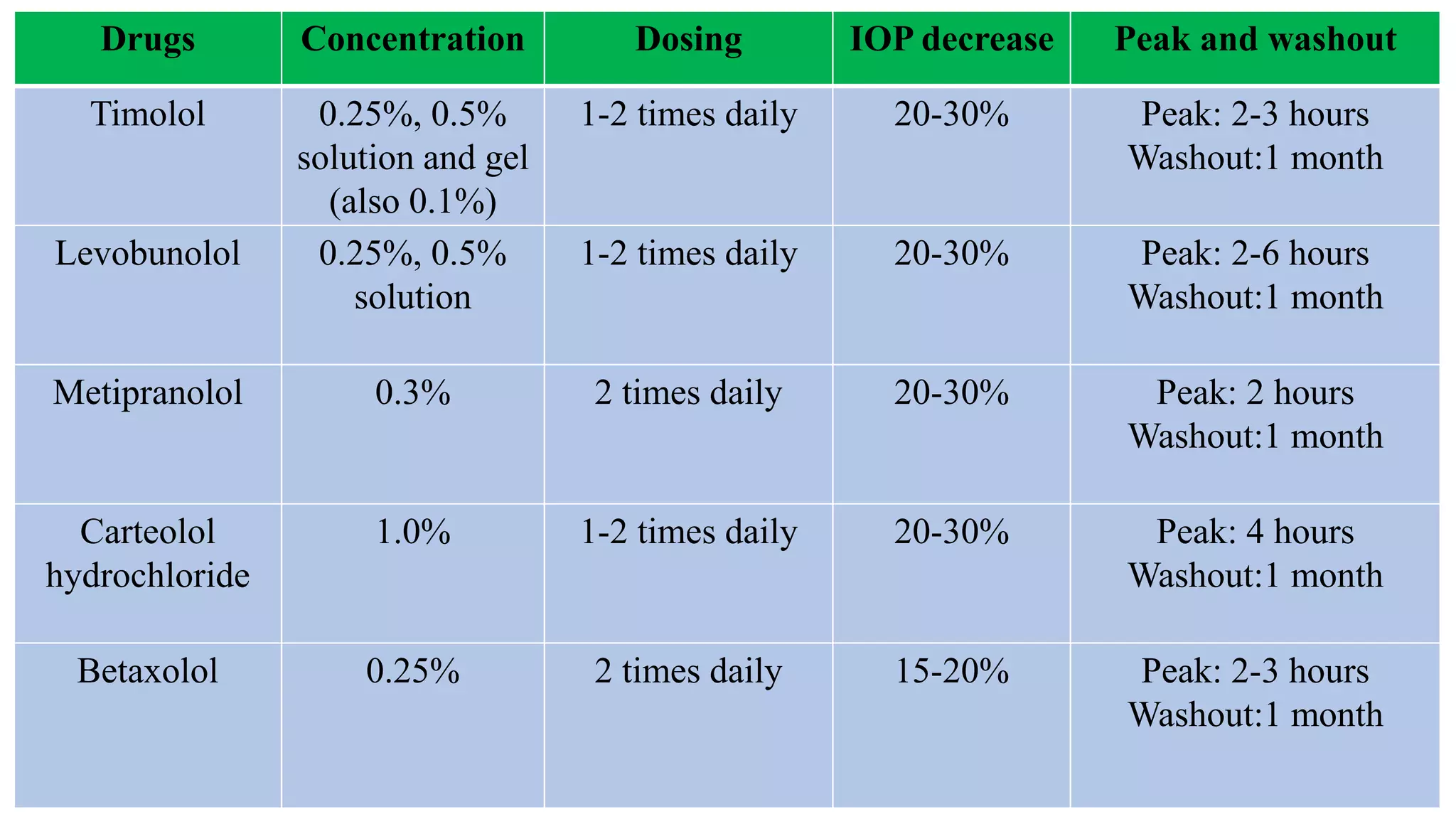
The document provides a comprehensive overview of pharmacotherapy for glaucoma, emphasizing the importance of reducing intraocular pressure (IOP) to prevent optic nerve damage and vision loss. It categorizes various drug classes used in glaucoma treatment, including prostaglandin analogues, β-adrenergic antagonists, α2 adrenergic agonists, carbonic anhydrase inhibitors, and parasympathomimetics, detailing their mechanisms of action, dosing, and side effects. The document also discusses target IOP calculations based on disease severity and outlines the therapeutic goals in managing glaucoma.