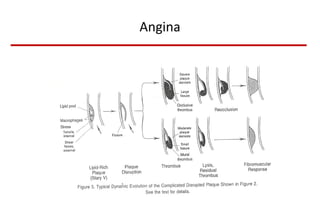
Angina pectoris, or chest pain, is caused by a lack of oxygen to the heart muscle. There are different types of angina including stable angina and Prinzmetal's angina. Treatment goals are to reduce symptoms and prolong life. Treatment options include medications like beta blockers, calcium channel blockers, and nitrates as well as lifestyle changes and procedures like angioplasty. Exercise testing can help evaluate ischemia and risk stratify patients.