Downloaded 107 times
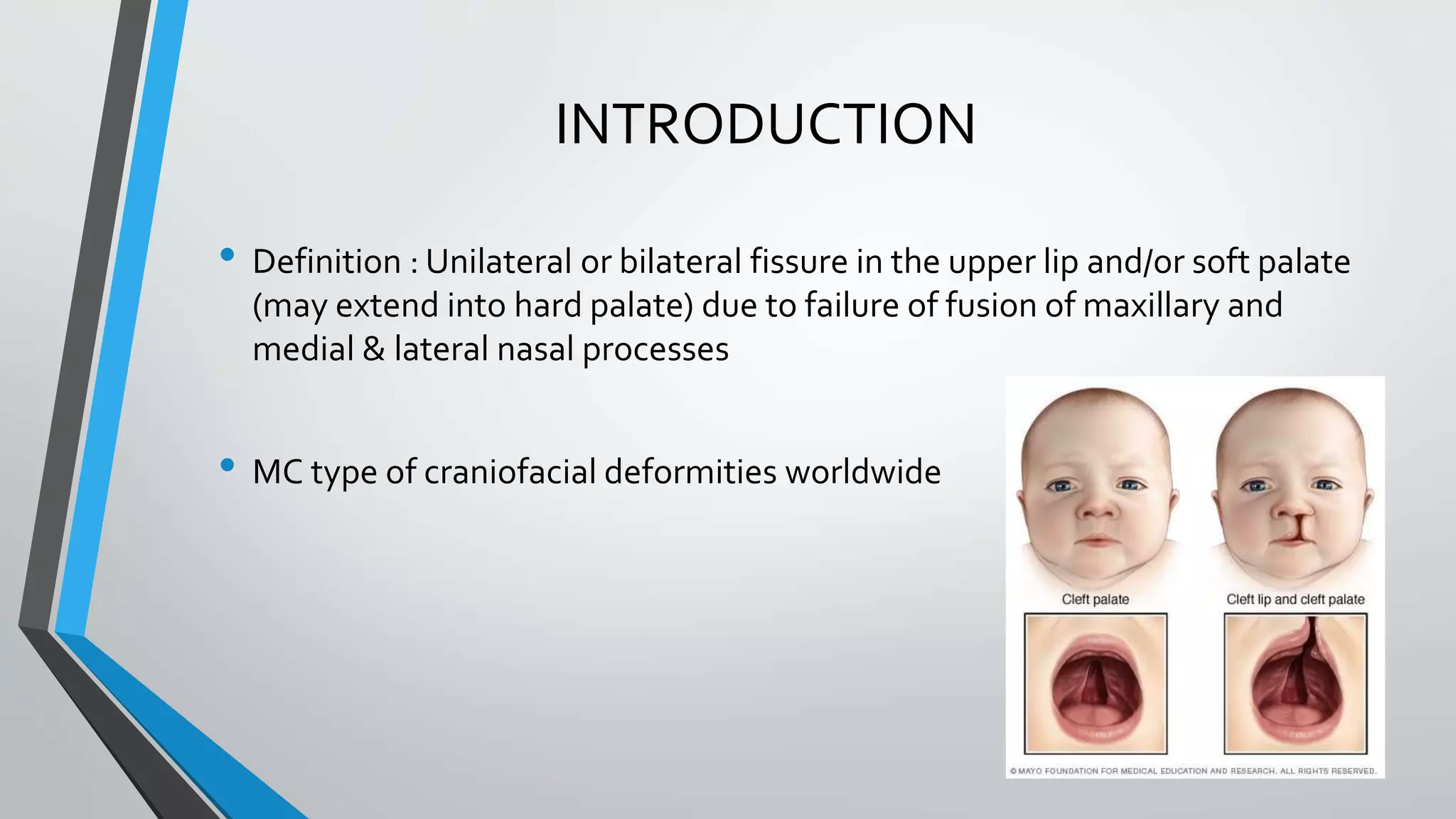






















- Cleft lip and cleft palate are congenital deformities caused by failure of facial structures to fuse properly during development in utero. - The document discusses the epidemiology, classifications, embryology, etiology, pathophysiology, associated conditions, timing of surgery, anesthetic concerns, and postoperative care for patients undergoing cleft lip and cleft palate repair surgery. - Key anesthetic considerations include the patient's young age, potential for a difficult airway, risk of multiple surgeries, shared airway with the surgeon, and potential for associated congenital anomalies.



































































