Downloaded 25 times
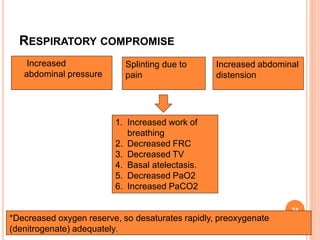


This document discusses anaesthesia considerations for emergency laparotomy in critically ill patients. Key points include: - Patients often present late with sepsis, dehydration, electrolyte imbalances, and respiratory compromise from abdominal issues. - Preoperative resuscitation is important to optimize the patient's condition through fluid resuscitation and correction of acidosis and electrolyte abnormalities over 2-4 hours. - During resuscitation, airway and breathing are prioritized through oxygen supplementation. Circulation is addressed through IV access and fluid administration while monitoring urine output and electrolytes. - Full preoperative optimization improves outcomes, but delays before surgery should be avoided in septic patients where early surgical management is beneficial











































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)










