Abdominal wall
• Abdomenis region between thorax and pelvic
cavity
• Extent is superiorly: diaphragm, inferiorly:
continous with pelvic cavity at pelvic inlet
• Anterior wall is by lower part of coastal
margin,external, internal oblique and tranversus
abdominis muscles, rectus abdominis and upper
part of pelvic bone
• Posterior wall is by quadratus lumborum,
iliopsoas, lumbar vertebrae and origin of
tranversus abdominis.
4.
Layers of anteriorabdominal wall
• Skin
• Superficial fascia: fatty (campers) and
membranous (scampers) layers
• Deep fascia
• Muscles
• Fascia tranversalis
• Extraperitoneal fat
• Parietal peritoneum
5.
Muscles of anteriorabdomen
External oblique
• Origin: lower eight ribs
• Insertion: xiphoid process, linear alba,
pubic tubercle, pubic crest, ant 2/3 of iliac
crest, lateral 2/3 of inguinal ligament
• Direction of muscle is downwards and
forwards
6.
Internal oblique
• Origin:lateral 2/3 of inguinal ligament, ant
2/3 of iliac crest and lumbar fascia
• Insertion: lower three ribs and their coastal
cartilages, xiphoid process, Linea alba,
symphysis pubis
• Direction of fibres: upwards and
backwards.
7.
Transversus abdominis
• Origin:lower six ribs and coastal cartilages
interdigitating with origin of the diaphragm,
lumbar fascia, ant 2/3 of iliac crest, lateral
1/3 of inguinal ligament.
• Insertion: xiphoid, linear alba, pubic
tubercle, syphsis pubis
• Direction of fibres: horizontal
8.
Rectus abdominis muscle:
•Origin: symphysis pubis, pubic crest
• Insetion: xiphoid, 5th
, 6th
and 7th
coastal
cartilages
• Nerve supply of anterior abdominal wall
muscles: ilioinguinal, iliohypogastric and
intercoastal nerves
• Fxns: respiration, protection, flexion of trunk,
forceful expulsion of fetus, flatus, urine, feaces
The gastrointestinal tract
•Extent: oral cavity to anal canal
• Parts: foregut, midgut and hind gut
• Foregut: composed of oesophagus, stomach and first
part of duodenum
• Midgut gut: rest of duodenum, ileum, jejunum, cecum,
appendix, ascending colon, proximal 2/3 of transverse
colon
• Hind gut: distal 1/3 of transverse colon, descending
colon, sigmoid colon, rectum and upper ½ of anal canal.
• Accessory organs namely pancreas, liver and spleen.
11.
Functions of thedigestive system
• Ingestion
• Digestion
• Absorption
• Egestion
12.
The fore gut
•Composed of oesophagus, stomach and first
part of duodenum
Oesophagus: muscular, collapsible tube, 25 cm
long connecting the pharynx to the stomach
• A passage of food from the oral cavity to the
stomach.
• Enters the abdomen by piecing the right crus of
the diaphragm at T10, and after a course of
2.5cm, it enters the stomach. Anteriorly is left
lobe of liver and posteriorly is the left crus of the
diaphragm. The right and left vagus lie posterior
and anterior to it.
13.
• Blood supplyof eosophagus: left gastric
artery
• Veins: left gastric veins
• Lymphatics: left gastric nodes, and finally
cealic nodes.
• Nerve supply: parasympathetics from left
and right vagi, sympathetics from
sympathetic trunk.
14.
Stomach
• Dialated partof the alimentary canal.
• Fxns: storage of food, mixes food with gastric
juices forming chyme, and release of chyme
into the duodenum.
• Structure: total capacity is 1500mls. In the
short and obese, it is high and transverse. In
the tall and thin, it is elongated and vertical.
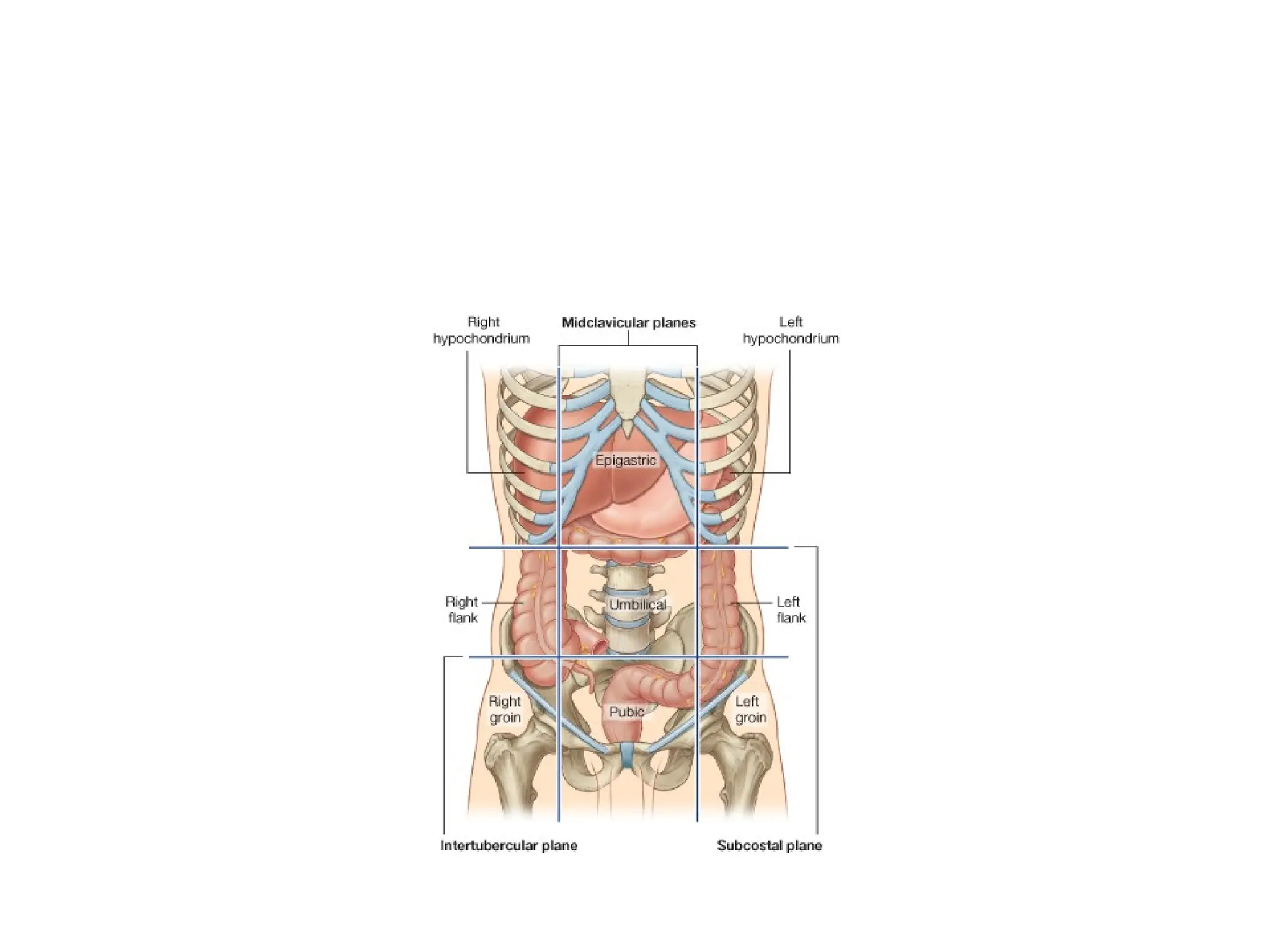
• It occupies the epigastric and umblical regions
and is under cover of costal diaphragm
15.
• It hastwo surfaces, two arpetures and two
carvetures.
• Surfaces: anterior and posterior surfaces
• Orifices: cardia and pyrolus
• Carvetures: greater and lesser carvetures
16.
• Cardia: ;locatedat eosophageogastric
junction. There is no anatomical sphincter but
a physiological sphincter formed by circular
layer of smooth muscles. This relaxes during
swallowing but closes after that to prevent
regurgitation of contents back into the mouth.
• Lesser curvature: located on the right margin.
Has attachments for the lesser omentum.
17.
• Greater curvature:located on the left margin
and has attachments for the gastrosplenic
ligament ( to spleen)and the greater omentum.
(to transverse colon)
• Anterior surface: has left vagal nerve running on
it.
• Posterior surface: has right vagal nerve on its
surface
• Pyrolus: located at the gastroduodenal junction.
18.
Parts of thestomach
• Has four parts: cardia, fundus, body and
pyrolus.
• Cardia: refer to above
• Fundus: dome-shaped and projects upwards
to the left of the cardia. Contains gas
• Body: extend from the cardia to the level of
insula angularis, a constant notch in the
lesser curvature.
19.
• Pyrolus: tubularpart of the stomach
connecting it to the duodenum. Has a thick
muscle wall called the pyrolic sphincter.
The cavity of the pyroluc is called the
pyrolus canal. It lies on the transpyrolic
plane(L1) and controls discharge of
stomach contents into the duodenum
20.
Mucous membrane ofthe
stomach
• Thrown into numerous fold called rugae.
These flatten when the stomach becomes
distended
• Muscle layer of the stomach: has three
layers: outer longitudinal, inner circular and
innermost oblique. The longitudinal are
mainly at the curvatures, the inner circular
sorround the stomach but are mainly at the
pyrolus and cardia.
21.
Peritoneum of thestomach
• The stomach is completely intraperitoneal.
It leaves the stomach as the lesser
omentum, greater omentum and the
gastrosplenic omentum.
22.
Relations of thestomach:
• anteriorly; anterior abdominal wall, coastal
margin, left lobe of liver, left pleura and
lung, diaphragm.
• Posteriorly:: lesser sac, diaphragm,
spleen, splenic artery, left kidney, left
suprarenal gland, pancreas, transverse
mesocolon and transverse colon.
23.
• Blood supplyof the stomach
• Left gastric: from cealic trunk. Supplies upper part
of lesser curvature
• Right gastric: from haepatic artery. Supplies lower
part of lesser curvature
• Left gastroepiploic: from splenic artery. Supplies
upper part of greater curvature
• Right gastroepiploic: from gastroduodenal(heaptic)
• Short gastric from splenic. Supplies fundus
24.
• Veins andlymphatics follow arteries.
• Nerve supply: anterior and posterior vagi
nerves and sympathetic trunk.
• Clinical notes:
• Trauma to the stomach: stomach relatively
mobile hence not usually injured except in
penetrating injuries like gunshot. Injuries lead
to peritonitis due to leakage of contents into
peritoneum.
25.
• Gastric ulcers:common at pyrolus and
lesser curvature where there is alkaline
producing mucosa. Can perforate.
• Gastric pain: reffered to the epigastrium via
sympathetic nerves.
• Cancer of the stomach: spreads to regional
nodes and surgery involves removal of all
regional nodes and neighbouring structures.
27.
Small intestines
• Longestpart of the alimentary canal.
Extends from the pyrolus to the ileoceacal
junction. involved in absorption of food.
• Divided into three parts: duodenum,
jejunum and ileum.
• Occupies mainly the epigastric, umblical
and hypogastric regions.
28.
Duodenum
• First partof the small intestines. 25 cm
long. First 2.5cm is intraperitoneal and
resembles stomach in structure as it is
covered by peritoneum on its anterior and
posterior surface, has lesser sac behind it,
attachments of lesser and greater omentum
to its wall.
• The remainder of the duodenum is
retroperitoneal
29.
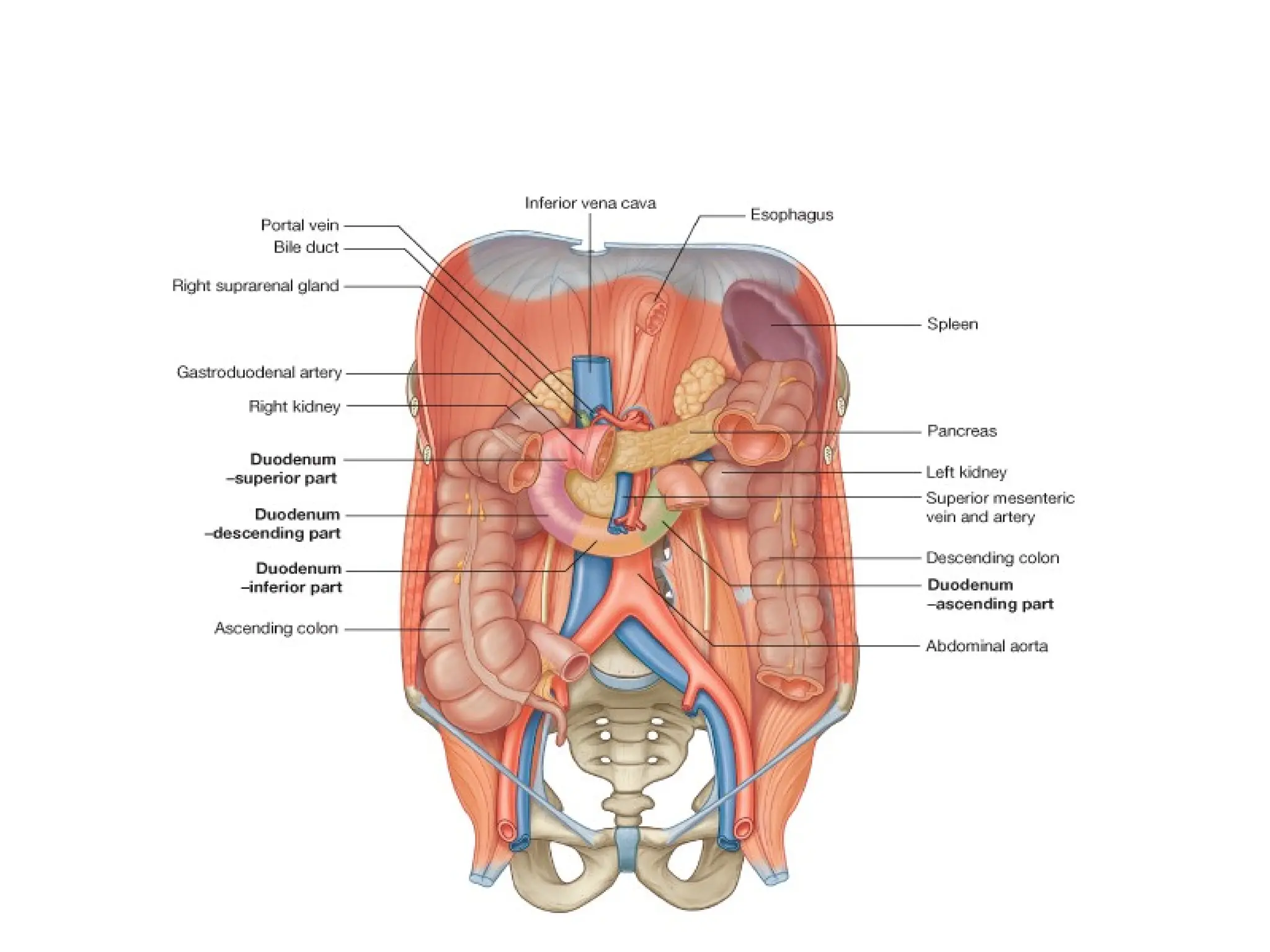
• The dudenumis c shaped and receives
openings of the bile duct and pancreatic
ducts
• It has four parts. part is 2 inches, 2nd
part
3 inches, 3rd
part 4 inches and 4th
part 2
inches long.
31.
First part ofduodenum
• 2 inches long, lies at the transpyrolic plane at
level of L1. first 2.5 cm similar to stomach. It
runs upwards and backwards to the right of L1
• Relations: posteriorly;lesser sac, bile duct,
poretal vein, gastroduodenal artery and IVC.
• Anteriorly: liver and gall bladder
• Superiorly: opening into lesser sac
• Inferiorly: head of pancreas.
32.
• Second partof duodenum: lies on the right of
L2 and L3 within the concavity of the head of
the pancreas. Receives the openings of the
bile duct and panctreatic duct.
Relations:
anteriorly;gall bladder, liver, coils of small
intestines and transverse colon
• Medially; head of pancreas, openings of
ducts
33.
• Laterally: ascendingcolon, right colic flexure
and liver
• Posteriorly: right kidney, psoas, right ureter,
aorta, IVC.
THIRD PART: runs horizontally to the left of
the subcostal plane.
• Relations: superiorly; head of pancreas,
inferiorly; coils of jejunum, posteriorly; aorta,
IVC, rightureter,psoas
34.
• Anteriorly: rootof mesentry of small
intestines with superior mesenteric artery
contained inside it and coils of jejunum.
• Fourth part: 2 inches long and runs
upwards to the left colic flexure. It is held by
ligament of treitz that is attached to the
diaphragm. It is related anteriorly to the root
of mesentry and coils of jejunum and
posteriorly to aorta and left psoas muscle.
35.
Jejunum and ileum
•They measure 6metres long with jejunum
being 2/5 while ileum is 3/5. each has
distinct features but there is a gradual
change as one moves from the jejunum to
the ileum.
• They are both suspended by a double layer
of peritoneum, the mesentry of small
intestines that is attaches from the right of
L2 to the sacroiliac joint
36.
Differences between ileumand
jejunum
• Jejunum occupies upper part of peritoneal
cavity to the left of the transverse mesocolon
while ileum is in the lower part to the right.
• It is redder, wider and thicker walled than the
ileum
• Its mesentry is attached to the posterior
abdominal wall above and to the left of the
aorta while that of the ileum is to the right and
below the aorta
37.
• Jejunal vesselsform only one or two arcades
that are long while ileal vessels form numerous
short arcades
• Peyers patches are present at the lower end of
the ileum along the antimesenteric border. These
are absent in the jejunum
• Fat deposition at the jejunal mesenteric border is
near the root and scanty at the intestinal wall.in
the ileum, it extends froom root of mesentry to
the intestinal border.
38.
• Blood supplyis from superior mesenteric
artery, veins and lymphatics follow
arteries.
39.
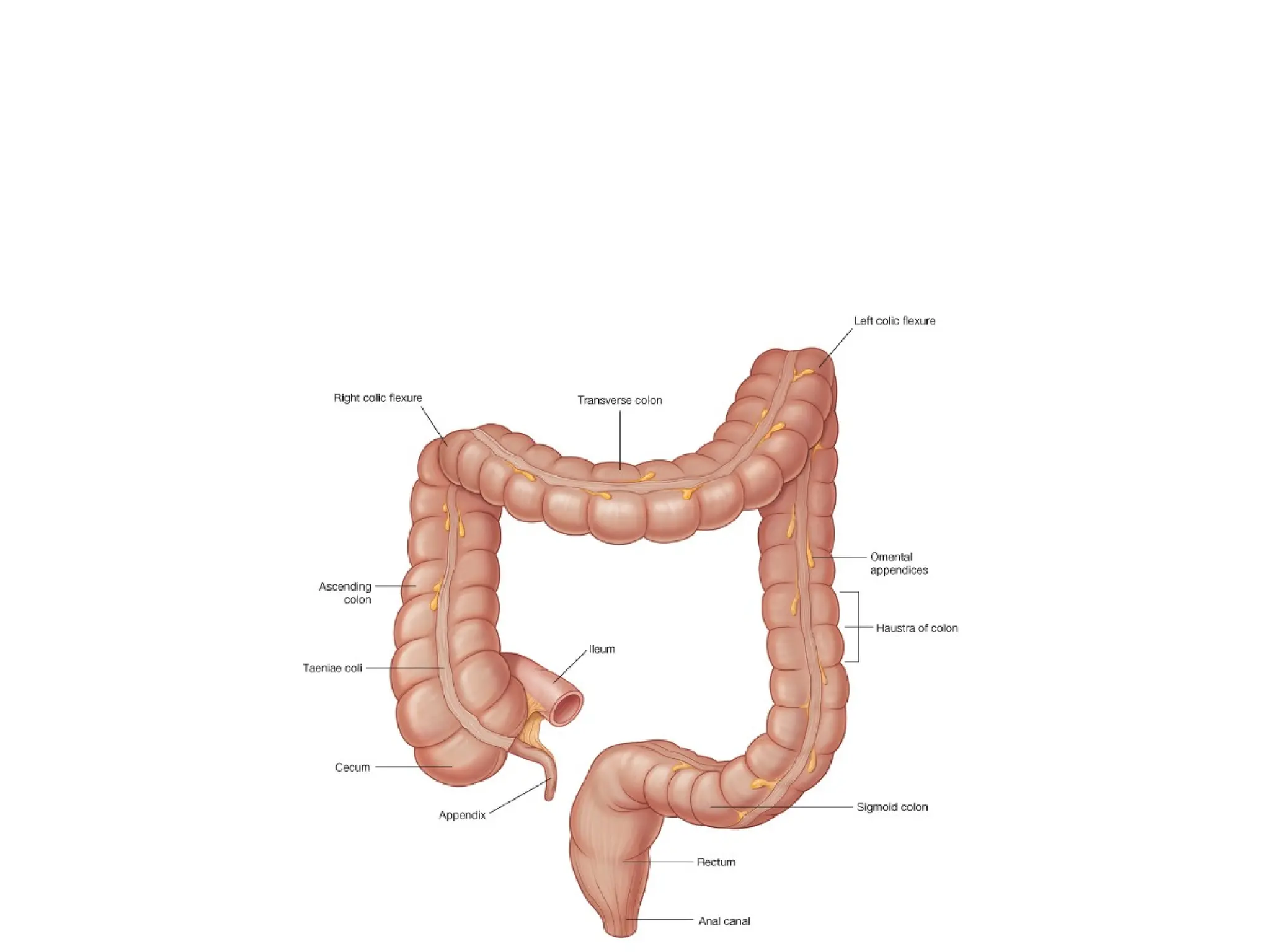
Large intestines
• Extendsfrom the ileum to the anus.
• Divided into ceacum, appendix, ascending
colon, transverse colon, descending colon,
sigmoid, rectum and anal canal
• Primary function is absorption of water and
electrolytes and storage of undigested
food substances till they are expelled from
the body as feaces.
41.
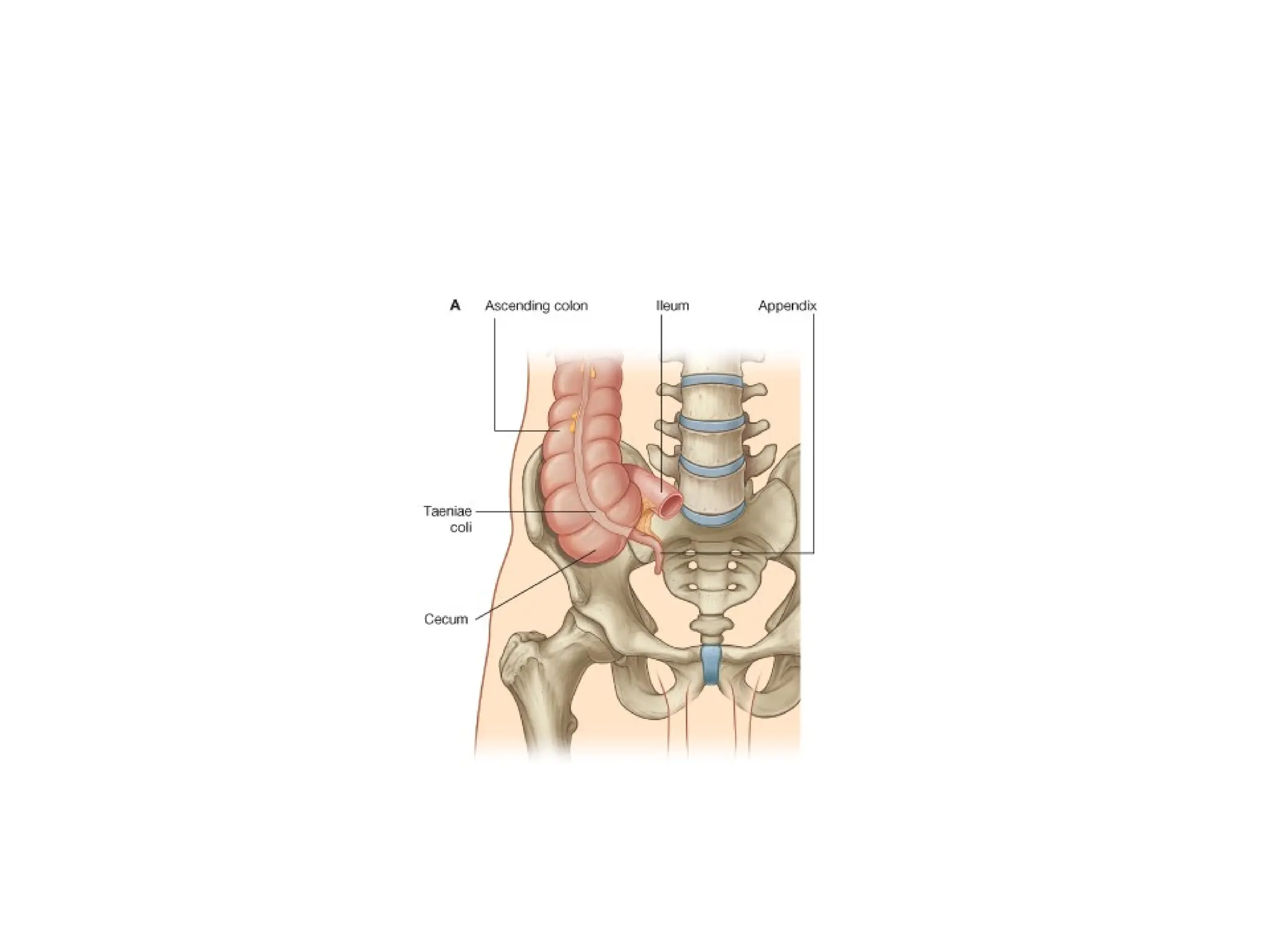
ceacum
• Part oflarge gut below level of junction of
ileum and large intestines. It is often
distended with gut and can be palpated in
the living individual. It is relatively mobile
though it lacks a mesentry. The three
longitudinal muscle layers form distinctict
bands called the Tenia Coli that converge
at the appendix.
42.
• Relations: anteriorly:abdominal wall, coils of
small intestines and greater omentum.
Posteriorly: psoas, femoral nerve, iliacus,
appendix, lateral cutaneous nerve of the
thigh.
• Blood supply: anterior and posterior
branches of the ileocolic artery, a branch of
superior mesenteric artery.
• Veins and lymphatics follow arteries.
43.
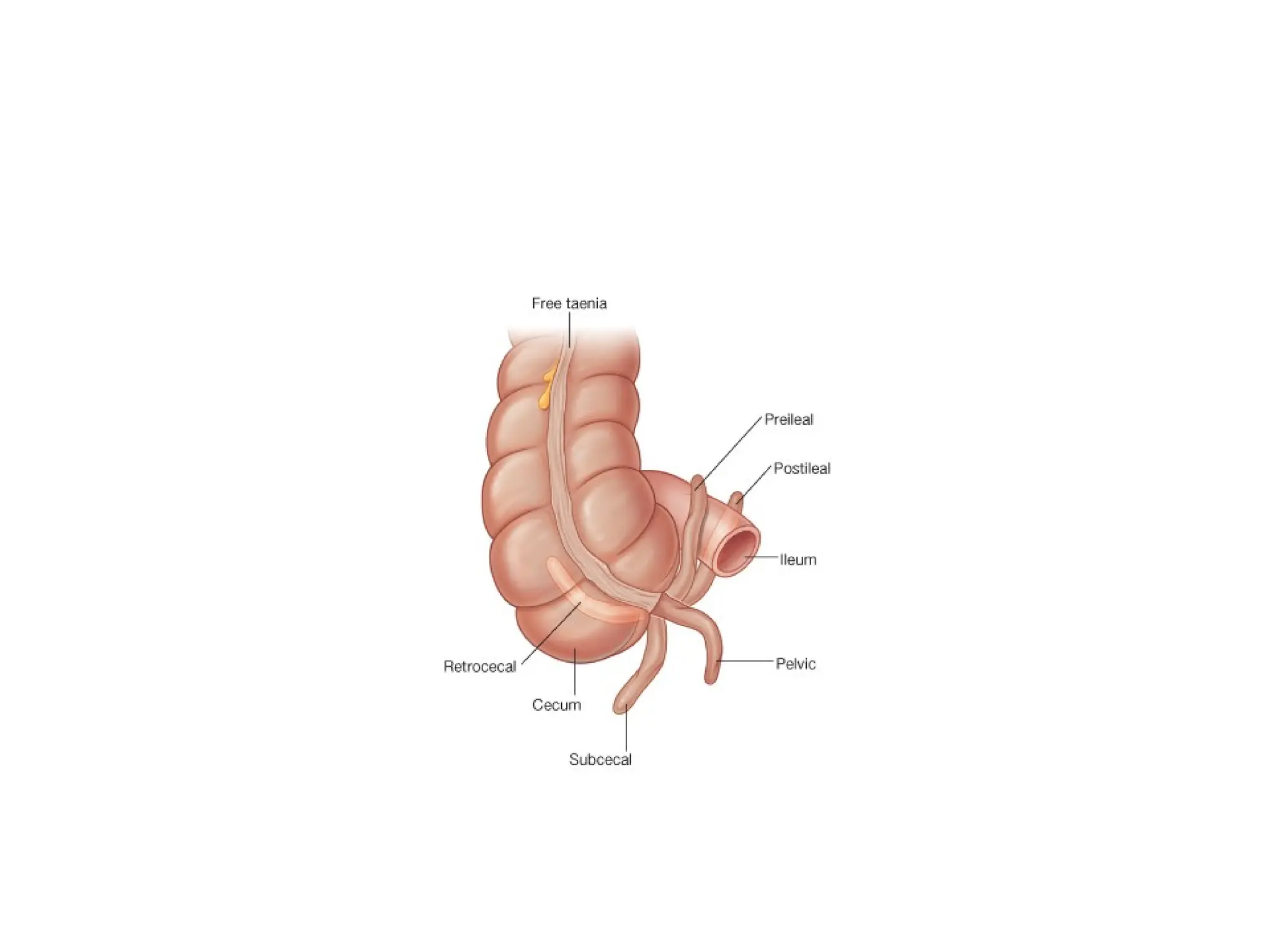
Vermiform appendix
• Anarrow musclural long tube containing a large
amount of lymphoid tissue. Varies in length from
8-13 cm. attached to the posteromedial surface
of the base of the cecum 2.5cm below the
ileocecal junction.
• Has a layer of peritoneum called the
mesoappendix
• Lies in the right iliac fossa 1/3 along the line
joining the ASIS and the umblicus(mc burney's
point)
44.
• Common positions:pelvic, retroceacal,
paraceacal, retro ileal.
• Blood supply: appendicular artery from
poaterior ceacal
• Veins and lymphatics follow arteries.
• N/S: Superior mesenteric plexus.
47.
Asending colon
• 13cm long, extending from the ceacum
above the ileocolic junction to the right colic
flexure. It is retroperitoneal
• Relations: anteriorly; anterior abdominal
wall, coils of small intestines, greater
omentum
• Posteriorly: ilopsoas, quadratus lumborum,
iliac crest, origin of transversus abdominis,
iliohypogastric and ilioinguinal nerves.
48.
• Blood supply:ilecolic and right colic from superior
mesenteric artery.
• Veins and lynmphatics follow arteries
• Transverse colon:38 cm long extending from the
right colic flexure to the left colic flexure. Has
greater omentum attached to its superior border
and transverse nesocolon attached to its inferior
border
• Relations: greater omentum and anterior
abdominal wall anteriorly
49.
• Posteriorly: duodenum,pancreas, colils of
ileum and jejunum
• Blood supply: proximal 2/3 middle
colic(SMA) distal 1/3 left colic(IMA)
• Veins and lymphatics follow arteries.
50.
Descending colon
• 25cm long extending from left colic flexure to
the sigmoid colon at the pelvic inlet.it is
retroperitoneal.
• Relations: anteriorly: coils of small intestines,
greater omentum and anterior abdominal wall.
• Posteriorly:left kidney, left psoas, spleen,
quadratus lumborum, ilioinguinal and
iliohypogastric nerves, femoral nerve, lateral
cutaneous of thigh, iliac crest
51.
• Blood supply:left colic(IMA)
• Veins and lymphatics follow arteries
52.
Sigmoid colon
• 25to 38 cm long and extends from the
pelvic brim as a continuation of the
descending colon and ends at level of S3.
• It has a mesentry making it relatively
mobile.
• Relations: anteriorly: uterus and upper part
of vagina in females, upper part of bladder
in males
• Posteriorly: sacrum,rectum, coils of ileum.
53.
• Blood supply:sigmoidal branches of
inferior mesenteric artery. Veins and
lymphatics follow arteries.
54.
Rectum
• 13 cmlong and extends from S3 as a continuation of the
sigmoid colon and ends infront of the coccyx by piercing
the pelvic diaphragm. The puborectalis muscle forms a
sling around the junction between the rectum and the
anal canal.
• The upper 1/3 is covered by mesentry on the anterior
and lateral surfaces, the middle 1/3 only on anterior
surface and lower 1/3 is devoid of peritoneum.
• The rectum follows the concavity of the sacrum.
• Mucosa and circular muscle layer folded to form
transverse folds of rectum. Longitudinal muscle layer
unites to form a single layer.
55.
• Relations: anteriorly;sigmoid colon, uterus and
vagina in females. Sigmoid colon, bladder,
prostate, seminal vesicles and vas deferens in
males
• Posteriorly: sacrum, coccyx, piriformis,
coccygeous, levator ani muscles
• Blood supply: upper 1/3 superior rectal(inferior
mesenteric), middle 1/3 middle rectal(internal
iliac), lower 1/3 inferior rectal(internalo
pudendal)
• Veins and lymphatics follow arteries
56.
Anal canal
• 4cm long,begins at level of levator ani
muscles and ends at the anus.
• Relations: posteriorly: anococcygeal body
• Laterally: ischiorectal fossa.
• Anteriorly: perineal body, urogenital
diaphragm, membranous urethra, and bulb
of penis in males. In females perineal
body, urogenital diaphragm and lower half
of vagina.
57.
Mucosa of analcanal
• Divided into upper and lower half
• Upper half is simple columnar, has anal
columns, supplied by superior rectal
nerves, arteries and veins. Lymphatics
end in inferior mesenteric nodes.
• Lower half is stratified squamous, has no
anal columns, supplies by inferior rectal
arteries, nerves and veins. Lymphatics go
to superficial inguinal nodes
58.
Anal sphincters
• Composedof involuntary internal and
voluntary external sphincters.
• Internal sphincter is a thickened layer of
circular muscle at upper end of anal canal
• External sphincter is composed of striated
muscle fibres of three parts namely
subcutaneous, superficial and deep.
• These control the expulsion of faecal
material from the gut.