Downloaded 51 times




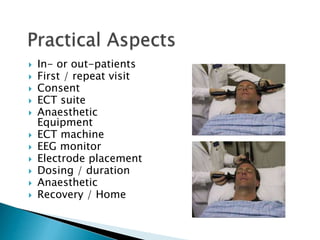











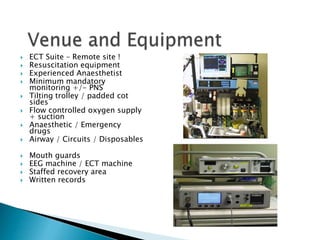













ECT involves inducing a seizure through brief electrical stimulation to treat severe mental illnesses. It was first developed in the 1930s and remains an effective treatment despite an unclear mechanism of action. Proper administration under anesthesia by an experienced anesthesiologist can minimize side effects and physiological responses while optimizing efficacy. Key considerations include patient assessment, appropriate monitoring and facilities, induction and recovery from brief general anesthesia without anticonvulsant drugs, and muscle relaxation to prevent injuries during the induced seizure.























































































