Outlines
• History
• Standardsfor basic anesthetic monitoring
• Introduction
• Capnography principle
• Types of capnograph
• Normal capnogram
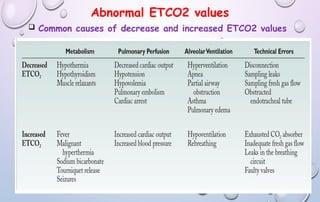
• Abnormal ETCO2 values
• Abnormal waveform.
• Capnography Vs Pulse Oximetry.
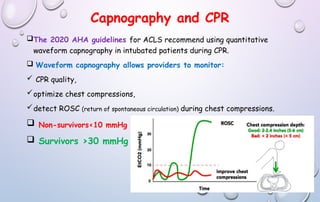
• Capnography and CPR.
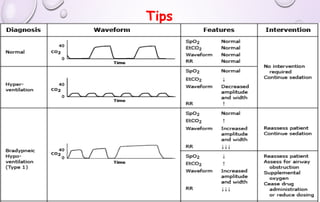
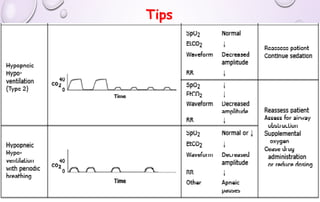
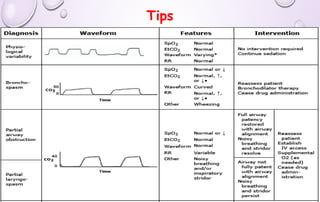
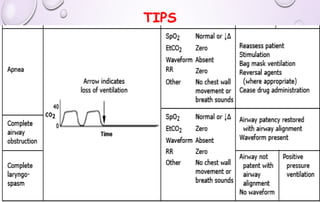
• tips
3.
History
In 1943,luft developed the principle of capnography based on the fact
that CO2 absorbs infrared light.
In the 1970s capnography was first studied clinically by smallhout and
kalenda in humans and has since been researched extensively.
By 1985, capnography was considered the standard of care for basic
anesthesia monitoring by the american society of anesthesiologists.
In the mid-1990s, co2 monitors (capnographs) became small and
inexpensive enough to be used in veterinary medicine
Capnography minimizes the need for repetitive arterial blood gas
sampling, thus providing an excellent noninvasive monitoring and diagnostic
tool.
4.
Standards for basicanesthetic monitoring
ASA standard II :
“During all anesthetics, the patient’s oxygenation, ventilation, circulation and
temperature shall be continually evaluated.”
“Every patient receiving general anesthesia shall have the adequacy of
ventilation continually evaluated.
Qualitative clinical signs such as chest excursion, observation of the reservoir
breathing bag and auscultation of breath sounds are useful.
Continual monitoring for the presence of expired carbon dioxide shall be
performed unless invalidated by the nature of the patient, procedure or
equipment.
Quantitative monitoring of the volume of expired gas is strongly encouraged.”*
• Developed by: committee on standards and practice parameters (CSPP)
last affirmed: december 13, 2020 (last amended october 20, 2010) (original approval: october 21, 1986)
5.
Introduction
Definitions
the termcapnography refers to the noninvasive measurement of the partial
pressure of carbon dioxide (CO2) in exhaled breath expressed as the
CO2 concentration over time.
The relationship of CO2 concentration to time is graphically represented by the
CO2 waveform, or capnogram
Capnography constitutes an important non-invasive technique that can continuously
monitors:
1. C02 production,
2. Pulmonary perfusion
3. alveolar ventilation.
4. respiratory patterns.
5. Cardiac output
6. Cellular metabolism
6.
Introduction
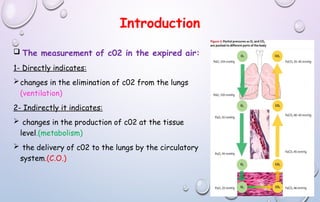
The measurementof c02 in the expired air:
1- Directly indicates:
changes in the elimination of c02 from the lungs
(ventilation)
2- Indirectly it indicates:
changes in the production of c02 at the tissue
level.(metabolism)
the delivery of c02 to the lungs by the circulatory
system.(C.O.)
7.
Capnography principle
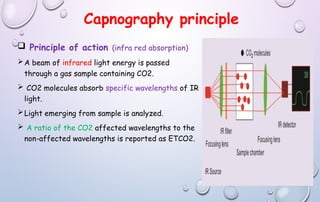
Principleof action (infra red absorption)
A beam of infrared light energy is passed
through a gas sample containing CO2.
CO2 molecules absorb specific wavelengths of IR
light.
Light emerging from sample is analyzed.
A ratio of the CO2 affected wavelengths to the
non-affected wavelengths is reported as ETCO2.
8.
Types of capnograph
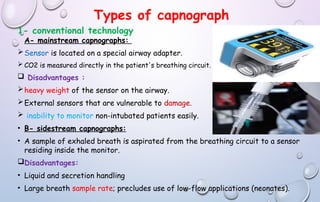
1-conventional technology
A- mainstream capnographs:
Sensor is located on a special airway adapter.
CO2 is measured directly in the patient's breathing circuit.
Disadvantages :
heavy weight of the sensor on the airway.
External sensors that are vulnerable to damage.
inability to monitor non-intubated patients easily.
• B- sidestream capnographs:
• A sample of exhaled breath is aspirated from the breathing circuit to a sensor
residing inside the monitor.
Disadvantages:
• Liquid and secretion handling
• Large breath sample rate; precludes use of low-flow applications (neonates).
9.
Types of capnograph
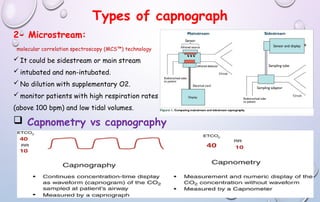
2-Microstream:
molecular correlation spectroscopy (MCS™) technology
It could be sidestream or main stream
intubated and non-intubated.
No dilution with supplementary O2.
monitor patients with high respiration rates
(above 100 bpm) and low tidal volumes.
Capnometry vs capnography
10.
Normal capnogram
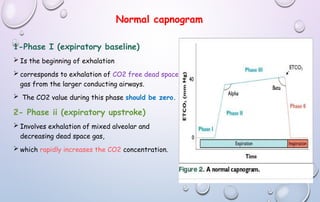
1-Phase I(expiratory baseline)
Is the beginning of exhalation
corresponds to exhalation of CO2 free dead space
gas from the larger conducting airways.
The CO2 value during this phase should be zero.
2- Phase ii (expiratory upstroke)
Involves exhalation of mixed alveolar and
decreasing dead space gas,
which rapidly increases the CO2 concentration.
11.
Normal capnogram
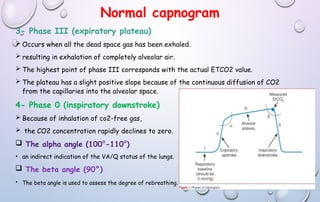
3- PhaseIII (expiratory plateau)
Occurs when all the dead space gas has been exhaled.
resulting in exhalation of completely alveolar air.
The highest point of phase III corresponds with the actual ETCO2 value.
The plateau has a slight positive slope because of the continuous diffusion of CO2
from the capillaries into the alveolar space.
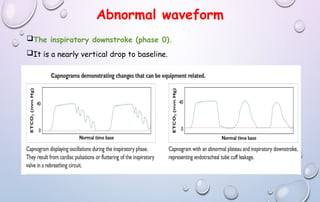
4- Phase 0 (inspiratory downstroke)
Because of inhalation of co2-free gas,
the CO2 concentration rapidly declinesto zero.
The alpha angle (100°-110°)
• an indirect indication of the VA/Q status of the lungs.
The beta angle (90°)
• The beta angle is used to assess the degree of rebreathing.
Abnormal waveform
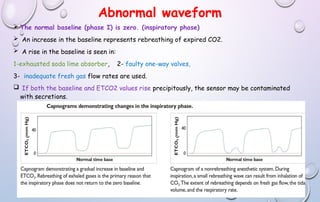
Thenormal baseline (phase I) is zero. (inspiratory phase)
An increase in the baseline represents rebreathing of expired CO2.
A rise in the baseline is seen in:
1-exhausted soda lime absorber, 2- faulty one-way valves,
3- inadequate fresh gas flow rates are used.
If both the baseline and ETCO2 values rise precipitously, the sensor may be contaminated
with secretions.
14.
Abnormal waveform
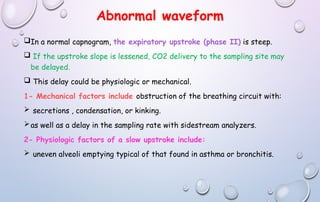
In anormal capnogram, the expiratory upstroke (phase II) is steep.
If the upstroke slope is lessened, CO2 delivery to the sampling site may
be delayed.
This delay could be physiologic or mechanical.
1- Mechanical factors include obstruction of the breathing circuit with:
secretions , condensation, or kinking.
as well as a delay in the sampling rate with sidestream analyzers.
2- Physiologic factors of a slow upstroke include:
uneven alveoli emptying typical of that found in asthma or bronchitis.
15.
Abnormal waveform
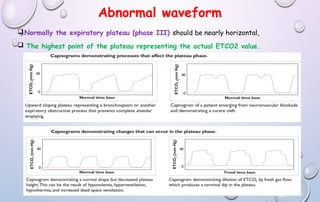
Normally theexpiratory plateau (phase III) should be nearly horizontal,
The highest point of the plateau representing the actual ETCO2 value.
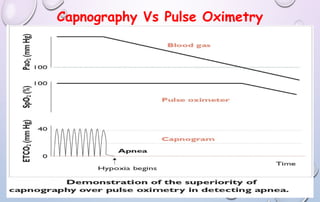
Capnography Vs PulseOximetry
ETCO2 has been shown to be superior to pulse oximetry in early detection
of airway mishaps, both technical and pathophysiologic.
It takes a longer time for oxygen saturation to drop compared with
changes in etco2.
Where the absence of co2 is detected instantaneously when the next
breath fails to occur.
Capnography can be used :
To confirm correct endotracheal tube and nasal esophageal feeding tube
placement.
Guide cardiopulmonary cerebral resuscitation (cpcr).
Assist treatment planning for patients receiving mechanical ventilatory
support.