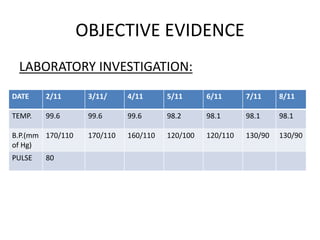
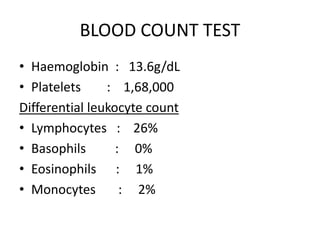
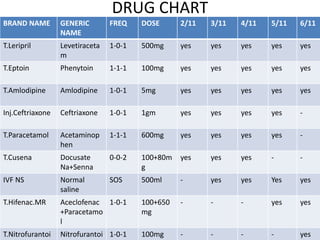
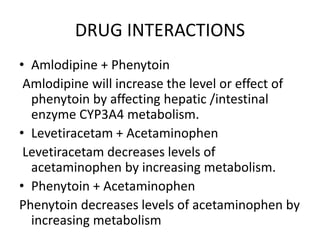
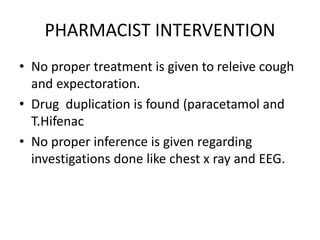
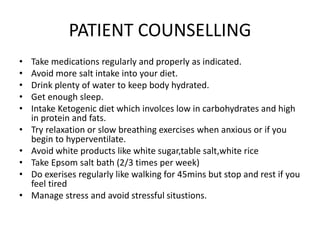
This document presents a case study of a 49-year-old male patient admitted to the hospital for generalized weakness, slurred speech, fatigue, fever, constipation, and cough for the past 3 days who has a history of epilepsy. Laboratory tests and investigations like CT scan and EEG were performed. Based on the subjective and objective evidence, the patient was assessed with epilepsy and hypertension. The goals of treatment were to relieve symptoms, control seizure frequency and severity, and improve quality of life. The patient's drug regimen and interactions are outlined, and the pharmacist notes duplication of paracetamol and lack of treatment for cough. The patient was counseled on medication adherence, diet, exercise, stress management, and lifestyle