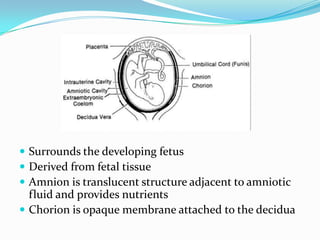


















The document discusses the characteristics and applications of amniotic membrane in ophthalmology, particularly for ocular surface reconstruction and corneal diseases. It describes the harvesting, preservation, and surgical techniques utilized, along with potential complications and indications for its use. The amniotic membrane's anti-inflammatory and healing properties make it a beneficial biological dressing in various ocular conditions.











































































































