






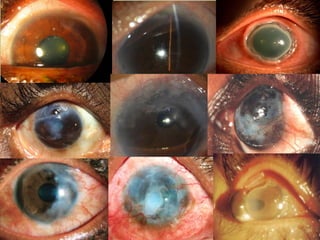



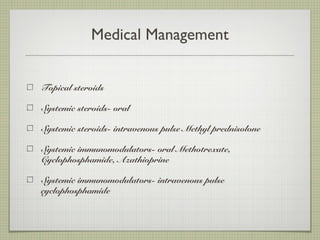






















Mooren's ulcer is a painful and aggressive form of peripheral ulcerative keratitis requiring multimodal management. The document details its demographics, etiopathogenesis, clinical features, and treatment strategies, emphasizing the importance of immunosuppression and a step ladder approach for therapy. Successful outcomes often necessitate both medical and surgical interventions tailored to disease severity.























































































