This document discusses eye banking and keratoplasty (corneal transplantation). It provides information on:
- The prevalence of corneal blindness in India and the role of eye banks in addressing the gap between donor cornea availability and demand.
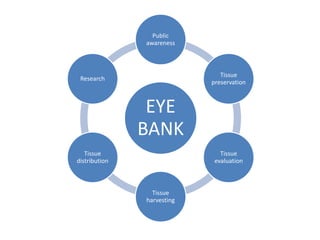
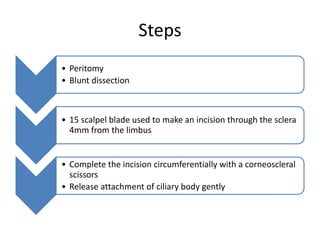
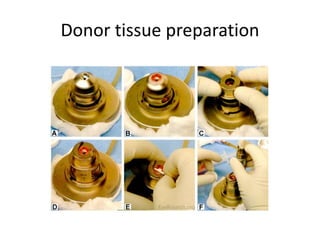
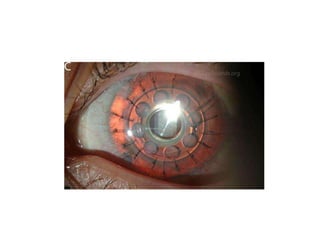
- The process of procuring, processing, evaluating and distributing donor corneas followed by eye banks. This involves coordinating with donor families, harvesting corneal tissue, examining tissue for suitability, and preserving and distributing corneas.
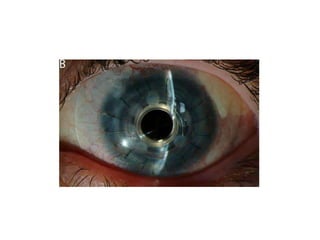
- Factors that are evaluated to determine suitability of donor corneal tissue including clarity, thickness, presence of scarring or edema, and endothelial cell density and morphology.
- Methods of preserving corneal tissue for short term, intermediate, long term storage




























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)


















