Downloaded 24 times
![WERNICKE-KORSAKOFF
SYNDROME [WKS]
Etiology
• Thiamine deficiency
• Encephalistis
• CO poisoning
• 3rd ventricle tumour
Wernicke
Encephalopathy
• Delirium
• Ophtalmoplegia
• Ataxia
• Peripheral neuropathy
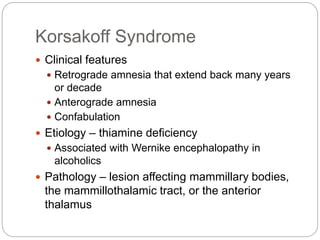
Korsakoff
Syndrome
• Amnesia
• Anterograde
• Retrograde
• Confabulation
Acute WKS: Mammillary body hemorrhages
Old WKS: Mammillary body atrophy
DSM-IV Alcohol-induced persisting amnestic disorder](https://image.slidesharecdn.com/amnesticdisorders2009-170704011201/85/Amnestic-disorders-2009-18-320.jpg)
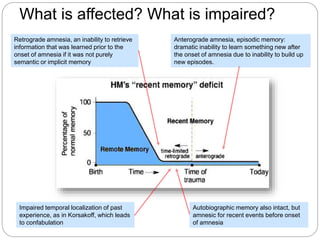
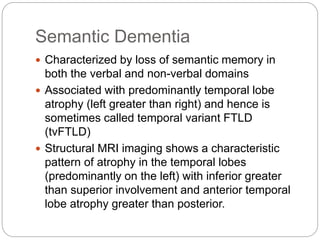
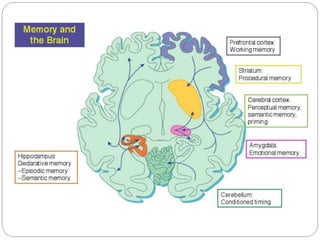


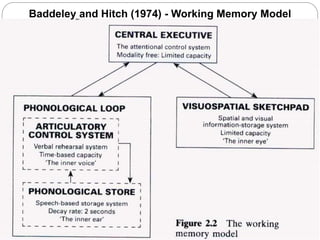
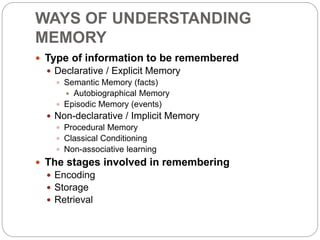
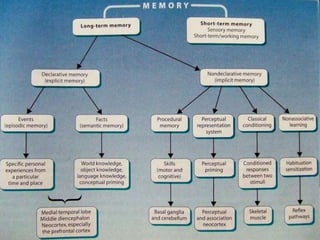
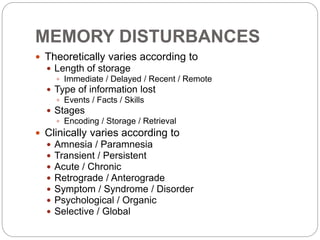
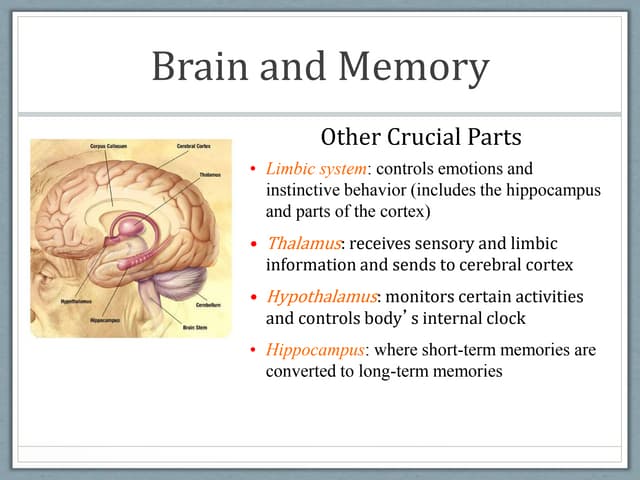
The document discusses various ways of understanding memory, including the length of storage, type of information remembered, and stages involved. It describes different memory models and then discusses various memory disturbances and disorders. Transient amnesias include transient global amnesia, transient epileptic amnesia, and alcoholic blackouts. Persistent memory disorders discussed include Korsakoff syndrome, herpes encephalitis, hypoxia, vascular disorders, and head injuries. Organic amnesic syndromes and their characteristics are also described.





![Amnestic disorders [2013]](https://cdn.slidesharecdn.com/ss_thumbnails/amnesticdisorders2013zo-170704024539-thumbnail.jpg?width=640&height=640&fit=bounds)









































![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)
![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)



![Non-delusional Morbid Jealousy [2019]](https://cdn.slidesharecdn.com/ss_thumbnails/56201795113132228753-190801100249-thumbnail.jpg?width=640&height=640&fit=bounds)




![Kesejahteraan Emosi di Tempat Kerja [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/kesejahteraanemosi2020-200905072541-thumbnail.jpg?width=640&height=640&fit=bounds)




























