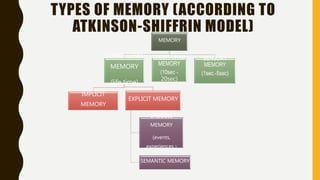
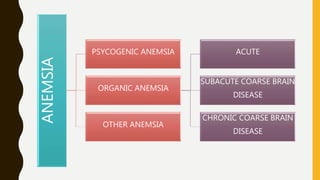
The document discusses memory and its stages including encoding, storage, and retrieval. It describes sensory memory, short-term memory, and long-term memory based on the Atkinson-Shiffrin model. It then discusses different types of memory impairment including amnesia, paramnesia, and hyperamnesia. Amnesia can be psychogenic or organic, with organic amnesia further divided into acute, subacute, and chronic forms based on the underlying brain disease. The document also discusses strategies to improve memory such as increasing oxygen to the brain and using cognitive strategies like elaboration, organization, and minimizing interference.







































![Amnestic disorders [2013]](https://cdn.slidesharecdn.com/ss_thumbnails/amnesticdisorders2013zo-170704024539-thumbnail.jpg?width=640&height=640&fit=bounds)














































