Download as PDF, PPTX
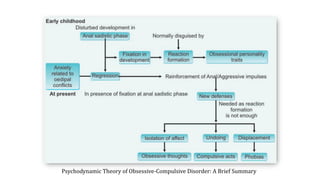
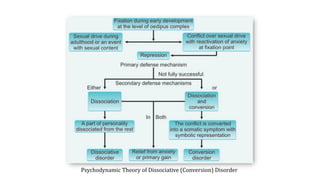
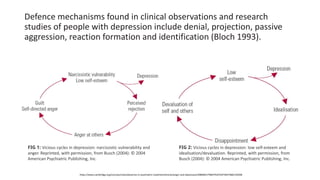

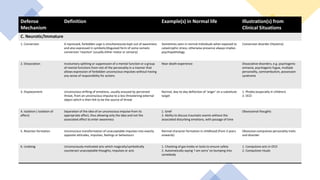
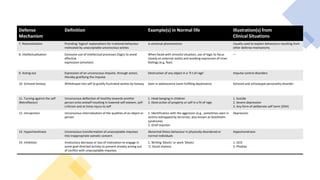
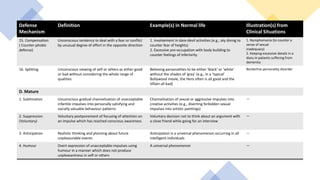
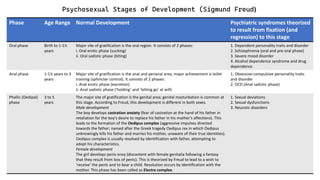


This document discusses psychodynamic theories of defense mechanisms and their relationship to psychiatric disorders. It provides a table outlining 16 common defense mechanisms like repression, projection, and rationalization. Examples of each in normal life are given along with illustrations from clinical situations. The document also summarizes Sigmund Freud's psychosexual stages of development from the oral phase to the genital phase and theorizes which psychiatric syndromes may result from fixation at each stage, such as schizophrenia from the oral phase or obsessive-compulsive personality traits from the anal phase.






















![Management of schizophrenia [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/managementofschizophreniaautosaved-201026030437-thumbnail.jpg?width=640&height=640&fit=bounds)






























![Kesejahteraan Emosi di Tempat Kerja [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/kesejahteraanemosi2020-200905072541-thumbnail.jpg?width=640&height=640&fit=bounds)
![Somatic Symptom and Related Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ssrdv1-200526002841-thumbnail.jpg?width=640&height=640&fit=bounds)
![Neurocognitive Disorders [2020]](https://cdn.slidesharecdn.com/ss_thumbnails/ncd2020v2-200526001756-thumbnail.jpg?width=640&height=640&fit=bounds)



![Non-delusional Morbid Jealousy [2019]](https://cdn.slidesharecdn.com/ss_thumbnails/56201795113132228753-190801100249-thumbnail.jpg?width=640&height=640&fit=bounds)



























