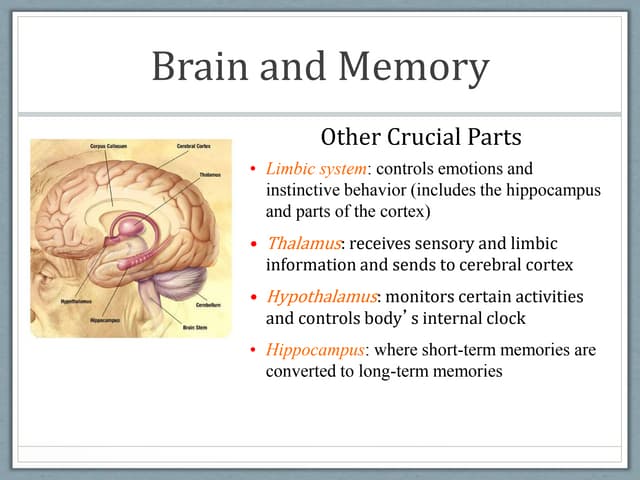
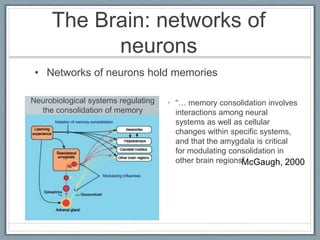
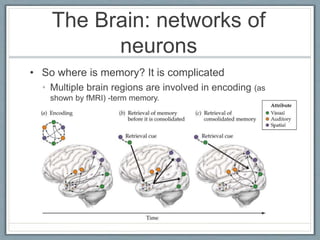
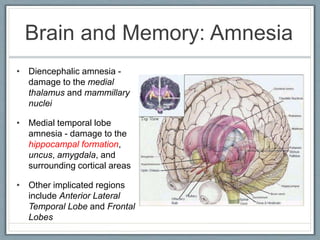
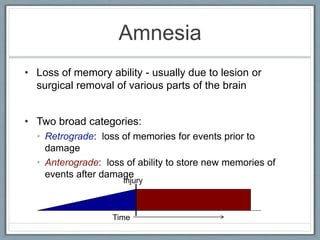
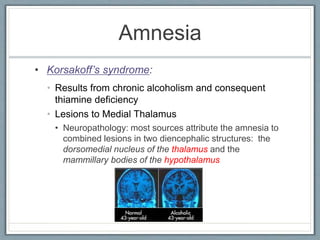
The document discusses memory and amnesia. It describes how memory is stored across multiple brain regions like the hippocampus, cortex, and amygdala. It explains different types of amnesia, such as Korsakoff's syndrome caused by thiamine deficiency, and post-traumatic amnesia caused by brain injuries. Retrograde amnesia involves inability to recall events before an injury, while anterograde amnesia impacts forming new memories after an injury. Famous amnesia cases like H.M. and Clive Wearing are also summarized.

















![60)NEUROBIOLOGY_OF_MEMORY[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/60neurobiologyofmemory1-231214020219-bfbe6909-thumbnail.jpg?width=640&height=640&fit=bounds)