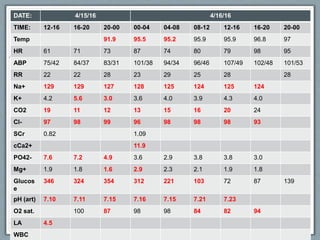
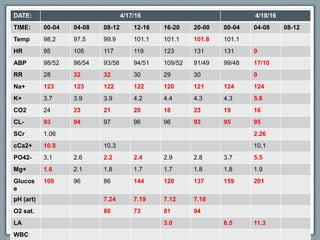
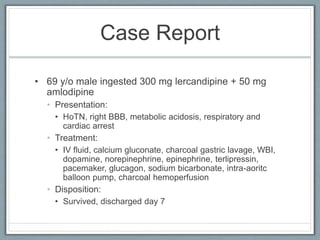
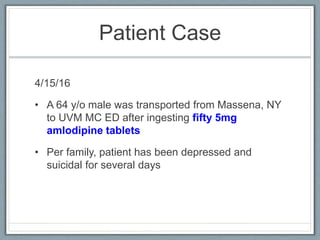
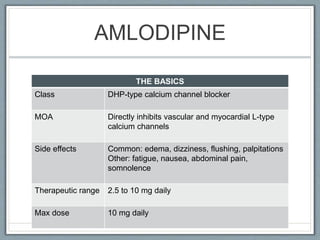
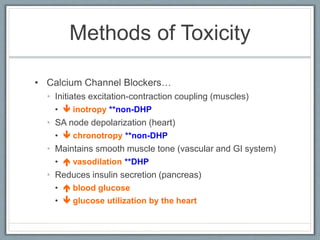
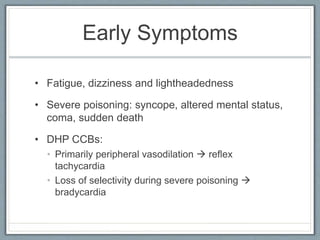
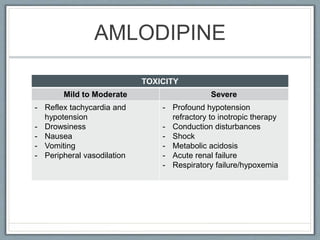
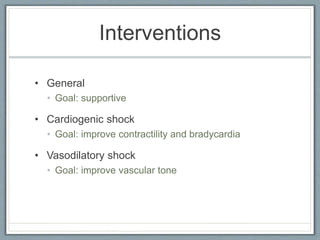
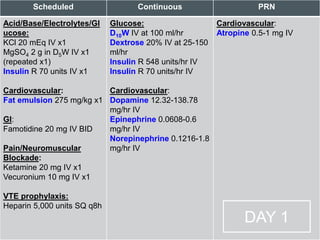
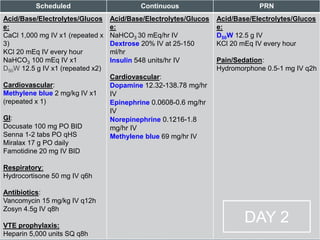
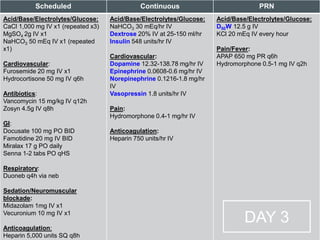
A 64-year-old male was brought to the emergency department after ingesting 50 tablets of amlodipine in a suicide attempt. Amlodipine is a calcium channel blocker that causes hypotension by vasodilation. The patient developed refractory cardiogenic and vasodilatory shock, metabolic acidosis, acute kidney injury, and other complications and did not improve despite multiple interventions. He was pronounced deceased on the fourth day of hospitalization.



![References
• Graudins A, Lee HM, Druda D. Calcium Channel Antagonists And Beta-Blocker Overdose: Antidotes and
Adjunct Therapies. British Journal of Clinical Pharmacology, 2015;81(3):453-461. doi: 10.111/bcp.12763
• Barrueto F. Calcium channel blocker poisoning. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA.
Accessed 01 May 2016.
• Hoffman RS, Howland MA, Lewin NA, et al. (2015) Goldfrank’s Toxocologic Emergencies, 10th Edition.
McGraw-Hill.
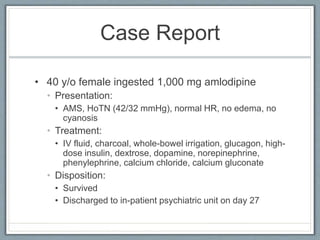
• Harris NS. Case 24-2006: A 40-Year-Old Woman with Hypotension after an Overdose of Amlodipine. N Engl J
Med 2006;355:602-611
• Nasa P, Singh A, Juneja D, et al. Continuous venovenous hemodiafiltration along with charcoal
hemoperfusion for the management of life-threatening lercanidipine and amlodipine overdose. Saudi Journal
of Kidney Diseases and Transplantation. 2014; 25(6):1255-1258.
• Kamp TJ, Hell JW. Regulation of Cardiac L-Type Calcium Channels by Protein Kinase A and Protein Kinase
C. Circulation Research. 2000;87:1095-1102.
• Clinical Pharmacology [database online]. Tampa, FL: Gold Standard, Inc.; 2016. URL:
http://www.clinicalpharmacology.com.](https://image.slidesharecdn.com/f48aad89-f45b-4144-9805-8335601655fa-160802033355/85/Amlodipine-Overdose-41-320.jpg)