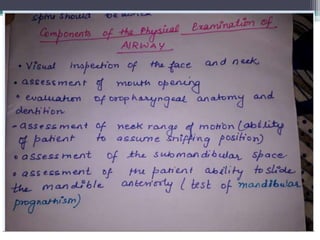
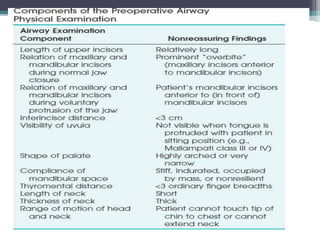
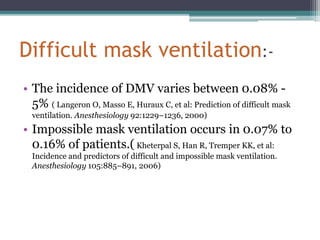
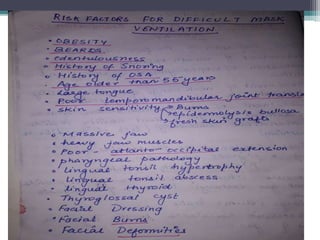
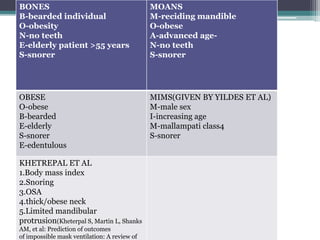
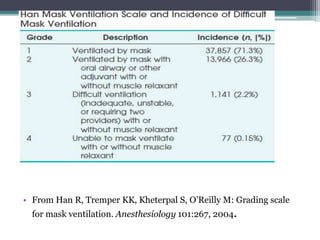
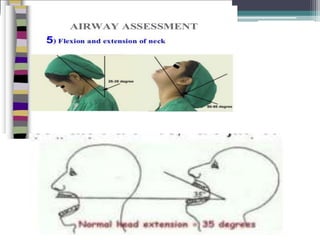
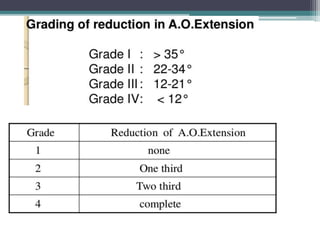
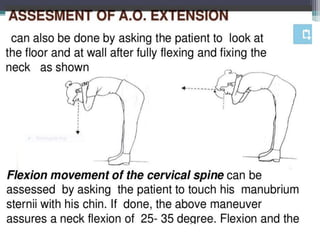
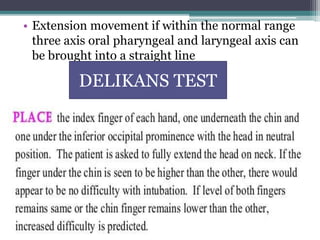
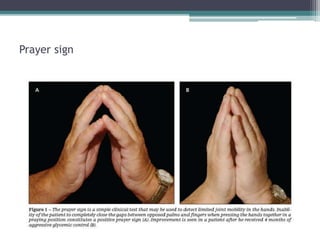
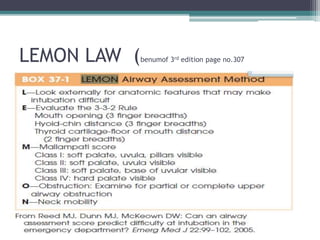
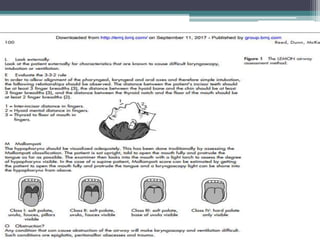
This document discusses methods for assessing a patient's airway for difficulty with mask ventilation, laryngoscopy, intubation, and a surgical airway. It describes various physical exam findings and grading scales that can help predict challenges, such as neck circumference, mouth opening, jaw protrusion, Mallampati score, thyromental distance, and laryngoscopic view with intubation. Factors like obesity, beard, lack of teeth, older age, and snoring increase risk. Proper airway assessment is important for anesthesia planning and preparing for potential difficulty.