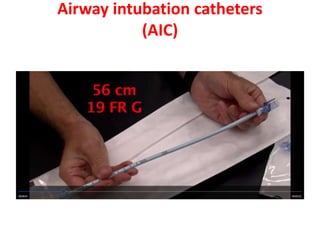
This document describes airway exchange catheters and the Aintree Intubation Catheter. Airway exchange catheters are long, thin, flexible catheters used to replace an endotracheal or tracheostomy tube already in place. The Aintree Intubation Catheter is an adaptation with a larger diameter that can be loaded onto a bronchoscope to guide placement of a new endotracheal tube after removing a supraglottic airway device. The catheter is inserted through the existing tube or supraglottic device and a new tube is railroaded over it. This allows visual guidance and avoids potential trauma from blind techniques. Risks include airway trauma, failure to insert the