Downloaded 195 times



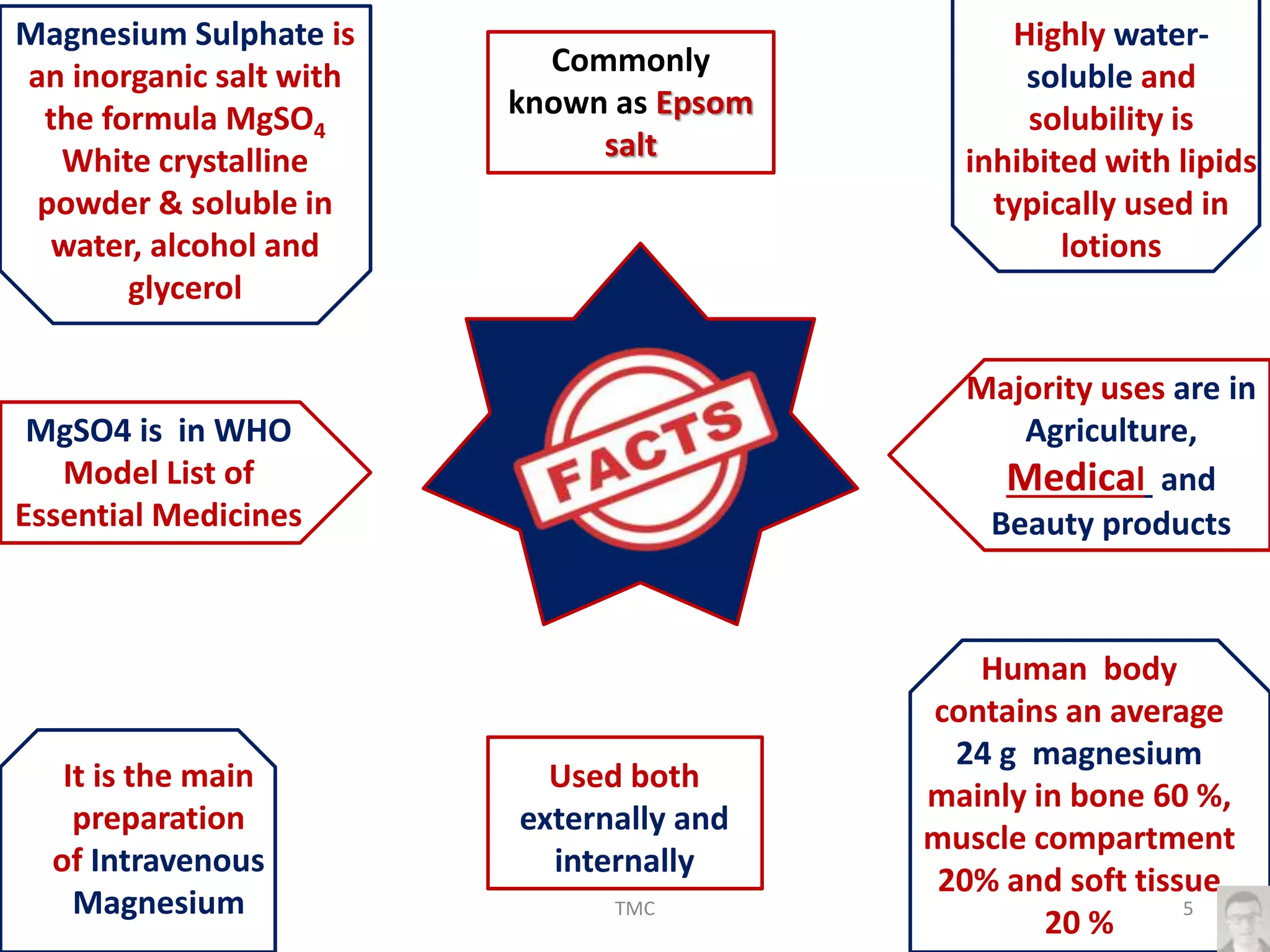
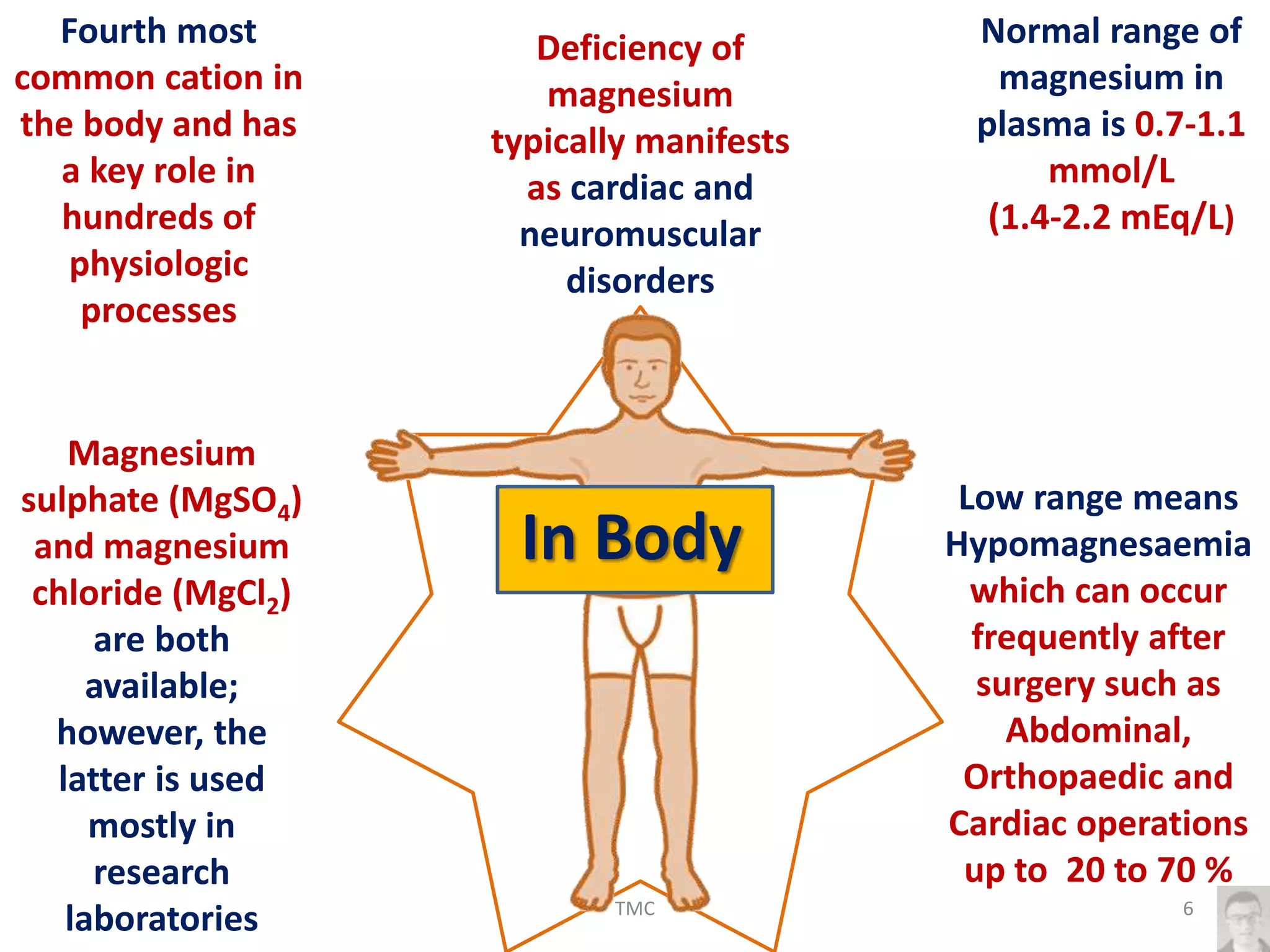

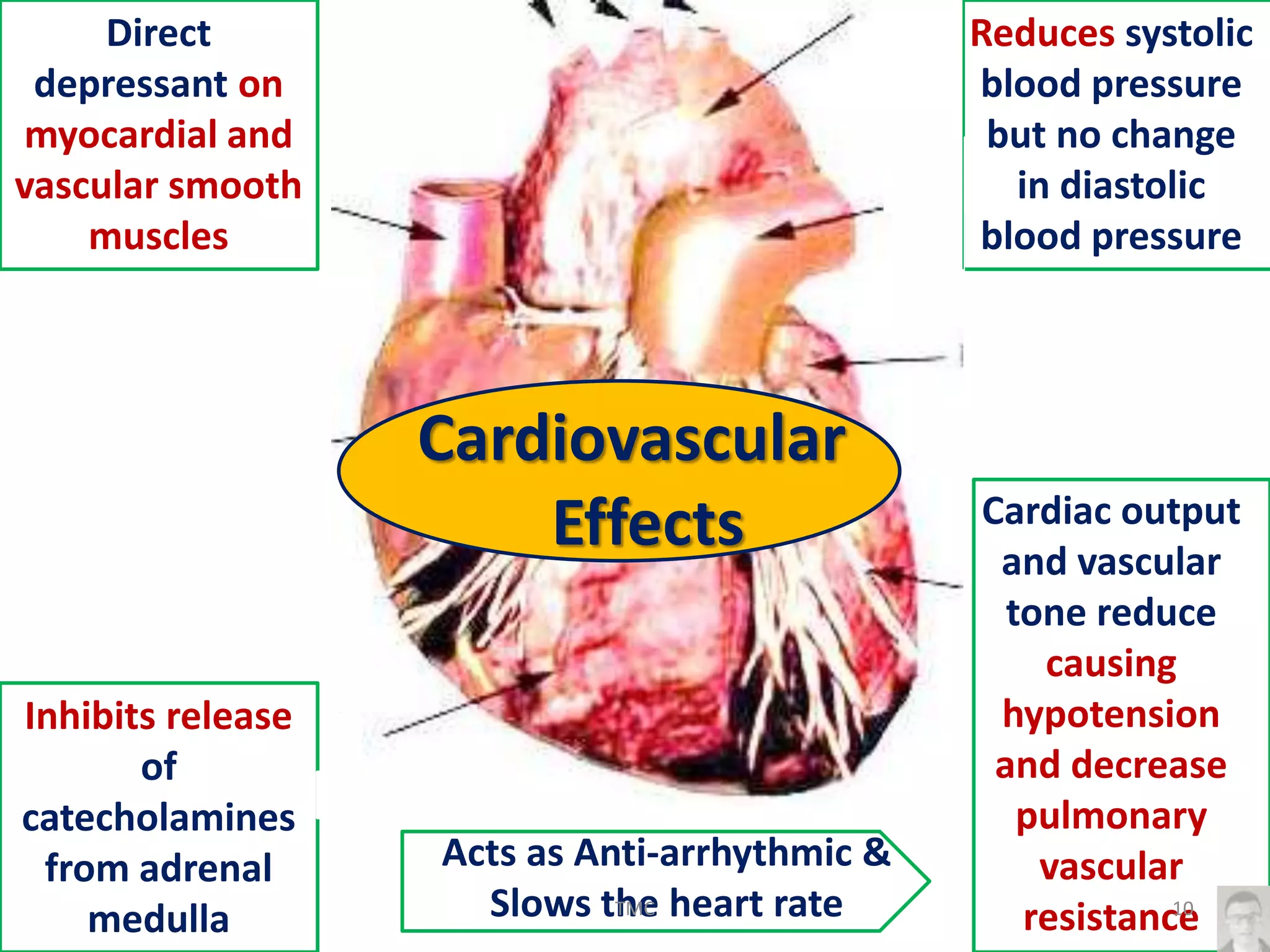


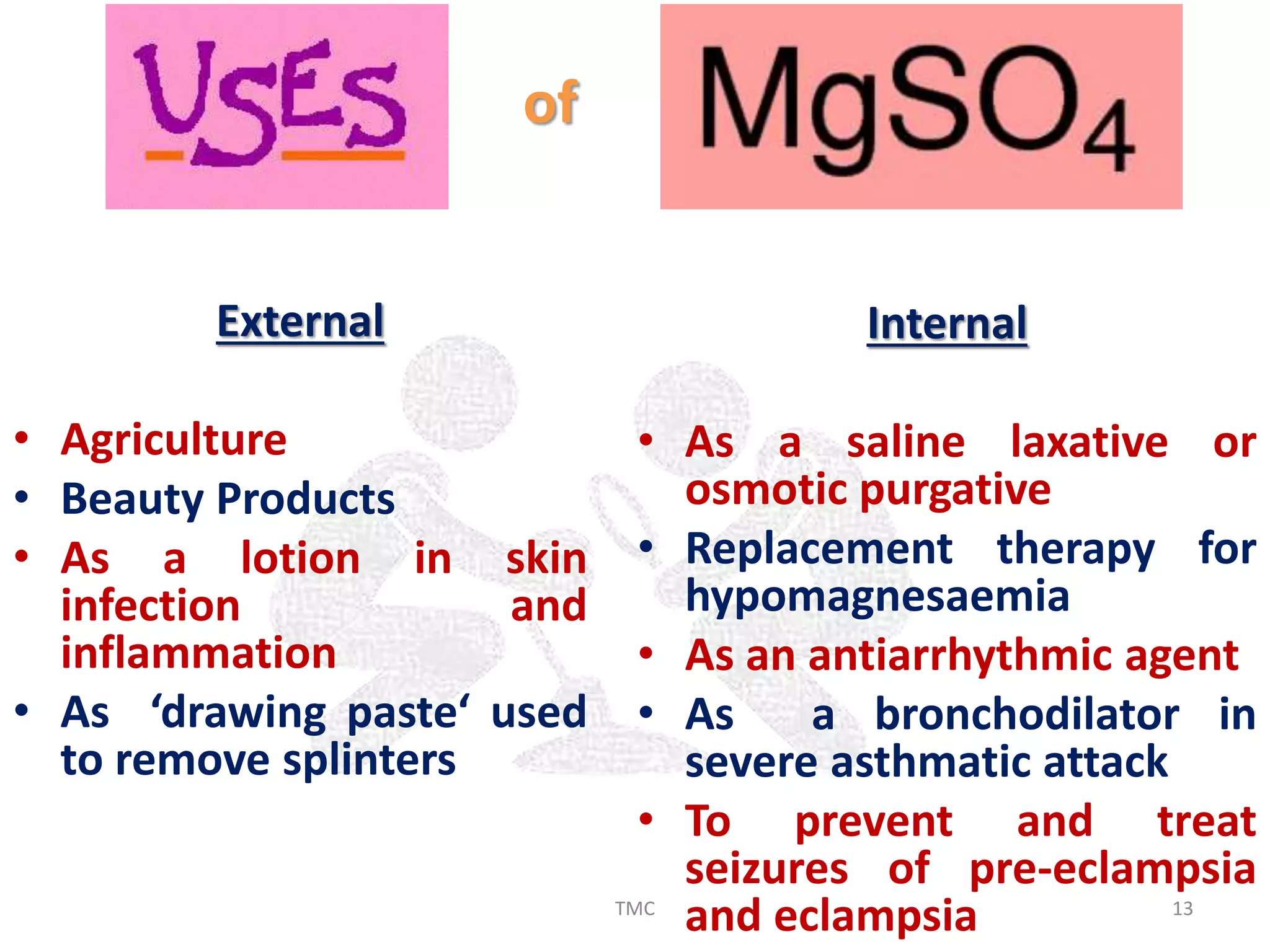





























The document discusses magnesium sulfate (MgSO4), including its history, physiological role in the body, systemic effects on different systems, uses in various medical contexts, administration, and experience with its use in anesthesia and analgesia. Magnesium sulfate has cardiovascular, neurological, musculoskeletal, and respiratory effects. It can be used to treat hypomagnesaemia, arrhythmias, preeclampsia, and more. Intravenous administration should be slow and side effects include burning, drowsiness, weakness, and respiratory issues in high doses. Magnesium sulfate may enhance the effects of anesthetics, muscle relaxants, and analgesics when used perioperatively.