Downloaded 122 times
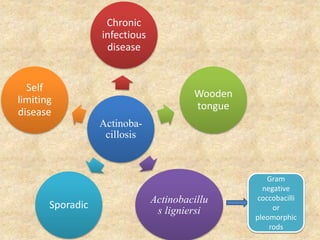
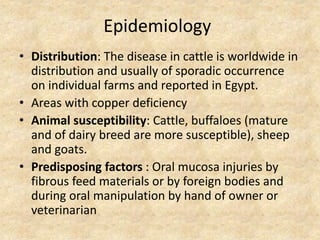
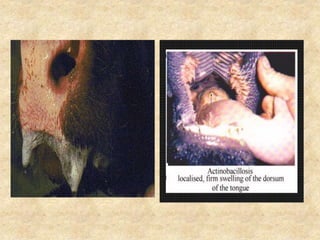

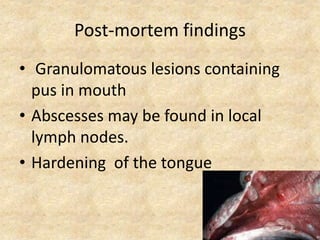

This document summarizes actinobacillosis, a chronic infectious disease caused by Actinobacillus lignieresi bacteria. It affects the tongues of cattle worldwide, especially in areas with copper deficiency. The bacteria are transmitted via ingestion of contaminated food or water by animals with oral injuries. Clinical signs include swollen tongues with nodules and ulcers that can cause pain and issues eating. Diagnosis involves finding the bacteria in samples. Treatment involves flushing wounds, potassium iodide, and antibiotics like streptomycin. Control relies on treating sick animals and preventing spread through isolation or disposal of those with lesions.