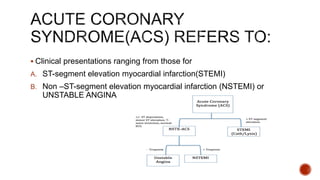
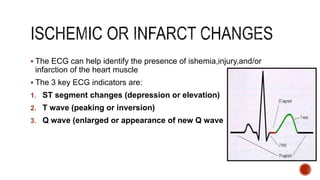
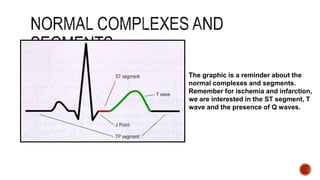
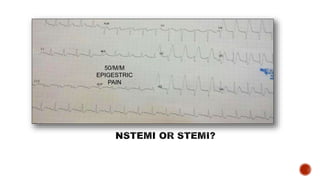
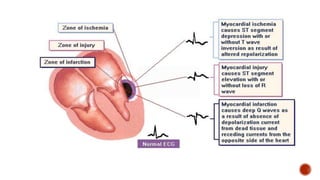
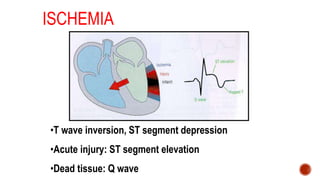
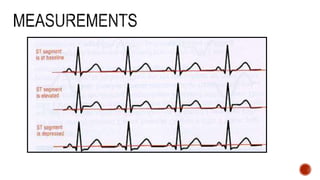
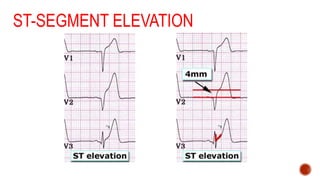
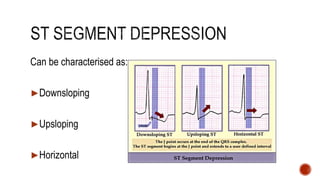
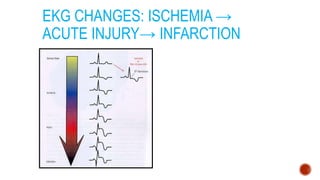
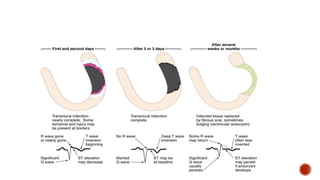
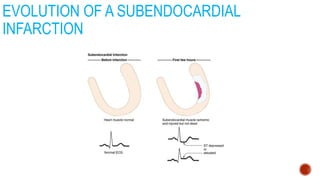
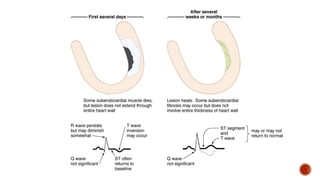
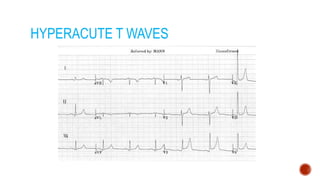
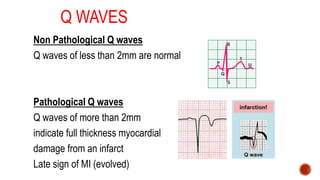
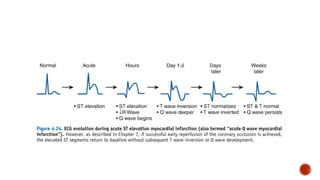
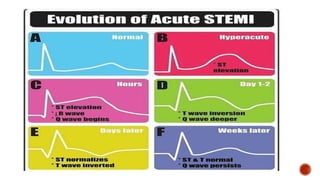
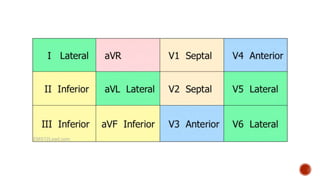
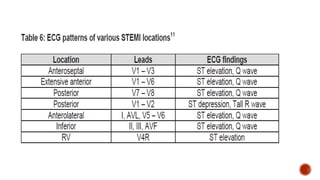
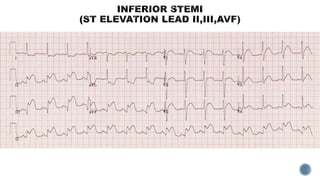
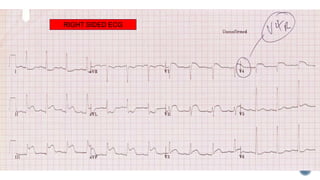
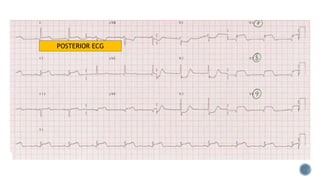
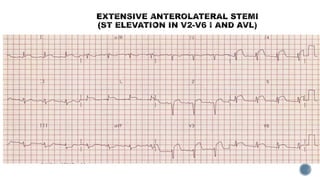
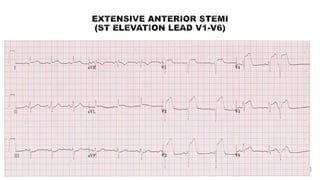
The document discusses ECG patterns that can help identify acute coronary syndromes including ST-elevation myocardial infarction (STEMI), non-ST-elevation myocardial infarction (NSTEMI), and unstable angina. Key ECG indicators of ischemia, injury, and infarction are ST segment changes, T wave changes, and presence of Q waves. ST elevation in two contiguous leads with chest pain symptoms indicates STEMI. The document provides guidance on cut-off points for ST elevation in different leads to diagnose STEMI and evaluating right ventricular involvement or posterior infarction. Repeating ECGs can help identify early changes in cases of suspected STEMI.