Downloaded 252 times

![How to Proceed?
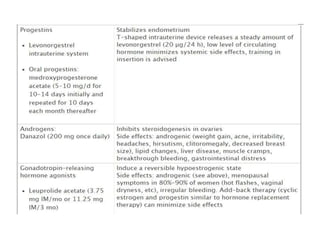
1. Primary Survey and Resuscitation1
2. History taking1,2,4,5
To identify the type of AUB [ovulatory (cyclical), anovulatory (irregular,
heavy), anatomical (e.g fibroids/polyps)]
Past obstetric/gynaecology history – fibroids, h/o myomectomy
Family history of cervical/endometrial ca.
Medications: ASA, Antidepressants, Anticoagulants, HRT, etc
3. Physical Examination1,2,4,5
To detect systemic involvements, mass per abdomen; pelvic and
bimanual examination must be done. Vaginal swabs TRO infections,
cervical cytology.](https://image.slidesharecdn.com/abnormaluterinebleedingss-140416003546-phpapp02/85/Abnormal-Uterine-Bleeding-AUB-13-320.jpg)
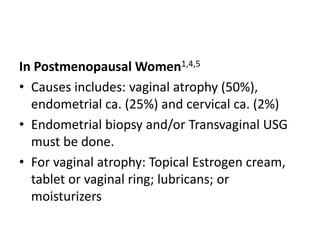
![Surgical Options1,4,5,6,7
• Endometrial ablation (laser, electrical, thermal or
radiofrequency energy) can be suggested [85% have
fewer symptoms].1,4,7
• Hysterectomy (permanent cure)1,5,7
• Uterine artery embolization and myomectomy can be
used for fibroids.1
• Dilation and Curettage (D&C) is no longer considered
as treatment.1](https://image.slidesharecdn.com/abnormaluterinebleedingss-140416003546-phpapp02/85/Abnormal-Uterine-Bleeding-AUB-25-320.jpg)



A 42-year-old teacher presented with menorrhagia for 6 months with lethargy and palpitations. On examination, she was pale with a pulse of 108 bpm. Investigations showed Hb levels decreasing from 8.1 to 7.8 g/dL. Ultrasound found an endometrial thickness of 6 mm without masses. She was diagnosed with dysfunctional uterine bleeding (DUB) and admitted for further management including IV fluids and iron supplements. DUB is abnormal bleeding due to hormonal imbalances that can cause heavy periods, and is diagnosed after excluding other causes. It is typically treated with hormonal therapy.



























































![ABNORMAL_UTERINE[1] DR SS NANda abnormal DA.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abnormaluterine1drssnanda-250706172120-db732f7a-thumbnail.jpg?width=640&height=640&fit=bounds)






































