Download as PDF, PPTX

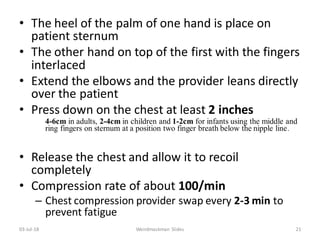
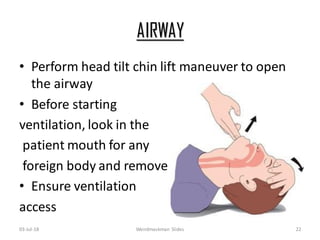
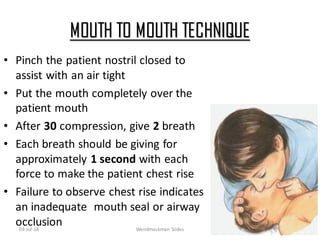
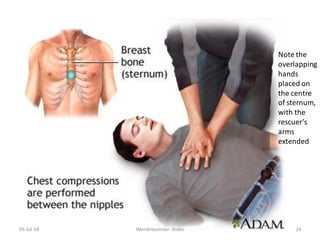
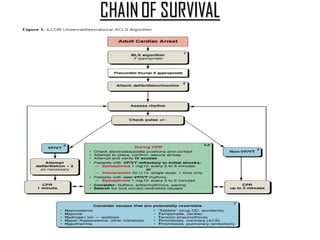
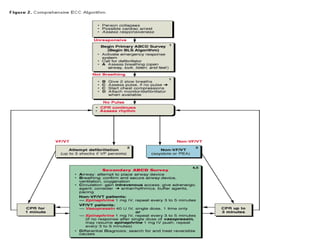
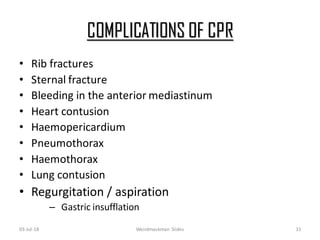

Cardiopulmonary resuscitation (CPR) has evolved over centuries from early techniques like applying heat or cold to more modern practices combining chest compressions and artificial ventilation. The document outlines the history and development of CPR, indications for its use in cardiac arrest, guidelines for techniques like chest compressions and airway management, and potential complications. Proper monitoring during CPR includes assessing pupils, pulse, breathing and consciousness to determine if resuscitation efforts should continue or be abandoned.



































































