Downloaded 90 times


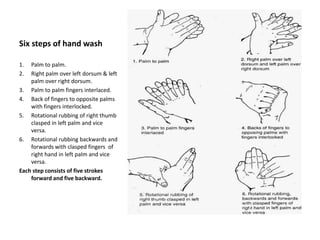

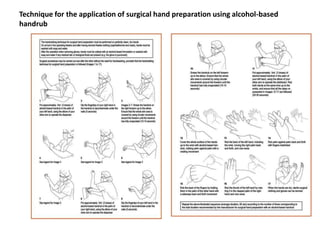

Hand washing is essential to prevent the transmission of infections. Proper hand washing procedures include wetting hands, applying soap, rubbing hands together for 20 seconds, rinsing with water, and drying hands. For surgery, a surgical hand wash is performed which includes washing hands and forearms with an antimicrobial soap, cleaning under fingernails, and scrubbing for 5 minutes. Alcohol-based hand rubs are preferred over soap and water in most situations due to their effectiveness and convenience. Correct hand hygiene is vital both for patient safety and the prevention of spread of antimicrobial resistance.