Downloaded 17 times
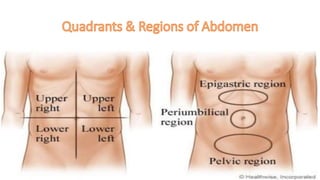
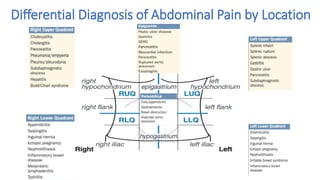
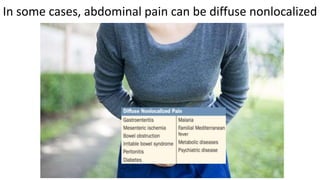
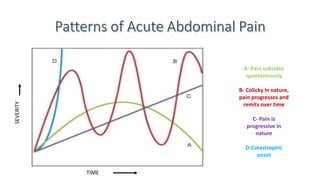
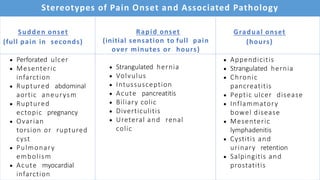


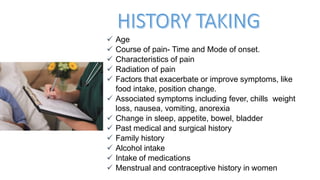
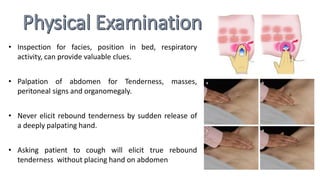
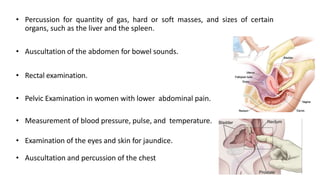



This document discusses the evaluation and differential diagnosis of abdominal pain. It notes that history and physical examination are important for diagnosis as subtle symptoms can indicate serious conditions. The document outlines key components of a patient's history and details the examination. It describes various causes of abdominal pain classified by location, mechanism, and onset. Radiological investigations that may assist diagnosis are also summarized. The document stresses that the severity of pain does not always correlate with the severity of the underlying condition.



































































