Downloaded 496 times


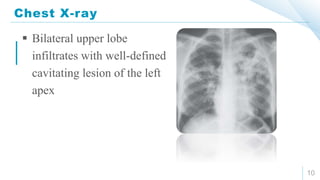





This document discusses three cases of tuberculosis (TB). The first case involves a 52-year-old Hispanic female presenting with cough, sputum, fatigue, and blood in her sputum. Examination finds lymph nodes and rales in her left lung. Tests show a positive PPD test and cavitary lesions on her chest X-ray, confirming active pulmonary TB. The second case is about a man referred for cough and fever, with bilateral pneumonia and apical involvement on chest X-ray. Sputum smear confirms acid-fast bacilli, and TB is diagnosed. He refuses admission and treatment. The third case discusses a woman diagnosed with sputum smear-negative pulmonary TB who stops treatment and attending follow























































































