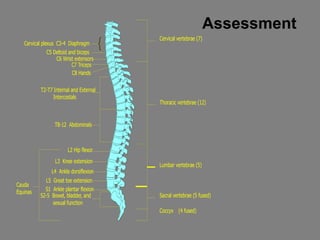
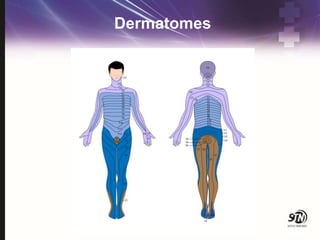
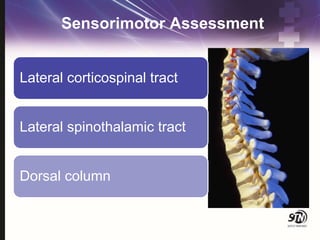
This document provides information on spinal cord and column injuries. It begins with objectives and epidemiology, then covers anatomy including the vertebrae, discs, ligaments, spinal cord and vessels. Mechanisms of injury are discussed as well as initial management including assessment, diagnostics, fractures/dislocations and SCIWORA. Long-term management includes prevention of respiratory, cardiovascular, gastrointestinal, urinary and skin complications. Musculoskeletal issues like spasticity, contractures and heterotrophic ossification are also addressed.













![9 Spinal Cord Injury Sci [2]](https://cdn.slidesharecdn.com/ss_thumbnails/9spinalcordinjurysci2-100330221058-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






































