ส�ำหรับอุปกรณ์เสริมในรองเท้านั้น มีการศึกษาเปรียบเทียบระหว่างแผ่นรองเท้าชนิด
พื้นเรียบ (flatinsole) กับอุปกรณ์พยุงส้นเท้าและฝ่าเท้าชนิดหล่อพิเศษเฉพาะราย (total contact
orthosis)พบว่าชนิดหลังช่วยลดแรงกดกระแทกที่ฝ่าเท้าได้ดีกว่าอย่างชัดเจน(79)
(คุณภาพหลักฐานIII)
ดังนั้น International Working Group on the Diabetic Foot ซึ่งเป็นหน่วยงานของสมาพันธ์
เบาหวานโลก แนะน�ำให้ใช้รองเท้าร่วมกับอุปกรณ์พยุงส้นเท้าและฝ่าเท้าชนิดหล่อพิเศษเฉพาะราย
เพื่อลดแรงกดกระแทกใต้ฝ่าเท้า ในขณะเดียวกันไม่แนะน�ำให้ใช้แผ่นรองเท้าชนิดพื้นเรียบหรือพื้นนุ่ม
ในการลดแรงกดกระแทกดังกล่าว(80)
(คุณภาพหลักฐาน IV)
อย่างไรก็ตามปัจจัยส�ำคัญในการป้องกันการเกิดแผลที่เท้าส�ำหรับผู้ป่วยเบาหวานนอกจาก
การใช้รองเท้าและอุปกรณ์เสริมในรองเท้าที่เหมาะสมและพอดีแล้ว สิ่งส�ำคัญอีกอย่างคือการดูแลเท้า
อย่างถูกต้องสม�่ำเสมอในชีวิตประจ�ำวัน(81)
ซึ่งรวมถึงการสวมใส่รองเท้าตลอดเวลาทั้งในและนอกบ้าน
จากการศึกษาพบว่าผู้ป่วยเบาหวานส่วนใหญ่สวมใส่รองเท้าในชีวิตประจ�ำวันเพียง 1 ใน 4 ของเวลา
งานเท่านั้น(82)
โดยปัจจัยที่อาจมีผลต่อผู้ป่วยเบาหวานในการที่จะสวมใส่รองเท้าหรือไม่นั้น ได้แก่
อายุ ความรับรู้ปัญหาสุขภาพและความผิดปกติของเท้า โรคประจ�ำตัวอื่นๆ รวมถึงความสวยงาม
ของรองเท้า(83, 84)
ดังนั้นแพทย์และบุคลากรทางการแพทย์ ควรเห็นใจและให้ความรู้ให้ผู้ป่วยเข้าใจ
ถึงประโยชน์และความส�ำคัญของการสวมใส่รองเท้าและอุปกรณ์เสริมในรองเท้า
8. บทบาทหน้าที่ของสถานพยาบาลและการติดตามการด�ำเนินงาน
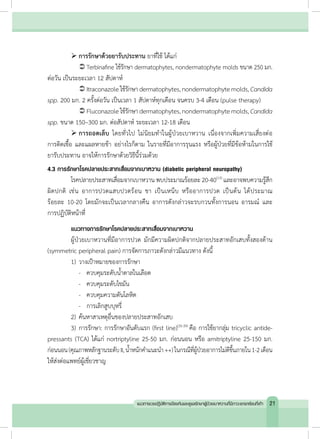
ข้อแนะน�ำ 13: การดูแลภาวะแทรกซ้อนที่เท้าในผู้ป่วยเบาหวาน ควรให้การดูแลอย่างต่อเนื่อง
โดยทีมดูแลป้องกันภาวะแทรกซ้อนที่เท้า และทีมสหสาขาวิชาชีพให้การรักษาผู้ป่วยที่มีแผลที่เท้า
และควรมีการก�ำหนดบทบาทหน้าที่ของทีมงานในหน่วยงานสถานบริการสาธารณสุขแต่ละระดับ
เพื่อการรับ/ส่งต่อผู้ป่วยอย่างเป็นระบบ (คุณภาพหลักฐานระดับ II, น�้ำหนักค�ำแนะน�ำ ++)
8.1 บทบาทหน้าที่ของสถานพยาบาล
ผู้ป่วยเบาหวานที่มีความเสี่ยงต่อการเกิดภาวะแทรกซ้อนที่เท้าต้องการการดูแลต่อเนื่อง
โดยอาจใช้กระบวนการดูแลผู้ป่วยเรื้อรังตามแบบของ Wagner’s Chronic Care Model (CCM)
และ WHO’s Chronic Care Model ในการสร้างเครือข่ายความร่วมมือในการดูแลผู้ป่วยแบบ
สหวิชาชีพอย่างรอบด้าน (multidisciplinary foot care team) ทั้งการป้องกันและรักษาโรค
การส่งเสริมสุขภาพกายและจิตใจ การฟื้นฟูผู้ป่วย มุ่งเน้นให้ประชาชนและชุมชนมีส่วนร่วม
เพื่อให้บรรลุเป้าหมายในการเข้าถึงทรัพยากรในการดูแลรักษาปัญหาภาวะแทรกซ้อนที่เท้า
ในผู้ป่วยเบาหวาน สถานบริการระดับต่างๆ จ�ำเป็นที่จะต้องมีบทบาทหน้าที่ชัดเจน สามารถจัด
เครือข่ายได้เหมาะสมตามทรัพยากรของสถานบริการ เพื่อพัฒนาไปสู่การดูแลปัญหาภาวะแทรกซ้อน
ที่เท้าร่วมกัน การจัดการดูแลผู้ป่วยที่มีภาวะแทรกซ้อนที่เท้าในแต่ละระดับ แสดงดังตารางที่ 8
34 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
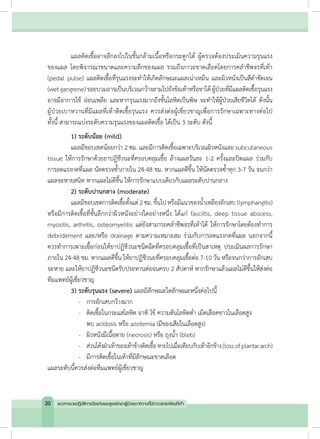
52.
ตารางที่ 8 บทบาทหน้าที่ของสถานพยาบาล
ระดับบริการ
ระดับที่1
ศูนย์เผ้าระวังสุขภาพ
เท้าเบาหวาน (primary
diabetic footcare
center)
ระดับที่ 2 ศูนย์
ป้องกันแผล
เบาหวานเท้า
(diabetic foot
protection
center)
ระดับที่ 3 ศูนย์ดูแล
แผลเบาหวานเท้าครบ
วงจร (comprehensive
diabetic footcare
center)
รพ. สต. รพช.
(ขนาดเล็ก)
รพท., รพช.
(ขนาดใหญ่)
รพศ. รพ.มหาวิทยาลัย
บุคลากร
เจ้าหน้าที่สาธารณสุข ü
พยาบาลเวชปฏิบัติ/พยาบาลวิชาชีพ
ที่ผ่านการอบรมหลักสูตรการดูแลเท้า
ในผู้ป่วยเบาหวาน
ü ü ü ü ü
Case manager ü ü ü
แพทย์เวชปฏิบัติทั่วไป ü ü ü ü
อายุรแพทย์ทั่วไป ü ü ü
อายุรแพทย์โรคต่อมไร้ท่อ ü ü
ศัลยแพทย์ทั่วไป ü ü ü
ศัลยแพทย์ตกแต่ง ü ü
ศัลยแพทย์กระดูกและข้อ ü ü ü
ศัลยแพทย์หลอดเลือด ü ü
แพทย์เวชศาสตร์ฟื้นฟู ü ü ü
แพทย์ผิวหนัง ü ü
รังสีแพทย์ ü ü
นักกายอุปกรณ์ (CPO or CPed) ü ü ü
นักโภชนาการ ü ü ü
บทบาท
ตรวจประเมินเท้า ü ü ü ü ü
ให้ความรู้ผู้ป่วยในการดูแลเท้า ü ü ü ü ü
รักษารอยโรคของเท้าที่ไม่ใช่แผล รักษาหรือ
ส่งต่อ
ü ü ü ü
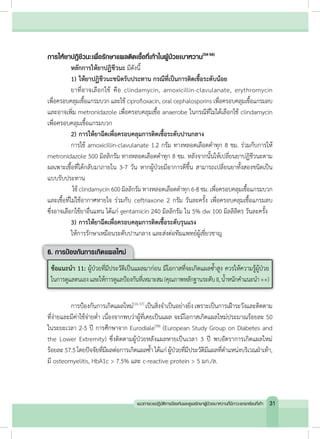
35แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
53.
ระดับบริการ
ระดับที่ 1
ศูนย์เผ้าระวังสุขภาพ
เท้าเบาหวาน (primary
diabeticfootcare
center)
ระดับที่ 2 ศูนย์
ป้องกันแผล
เบาหวานเท้า
(diabetic foot
protection center)
ระดับที่ 3 ศูนย์ดูแล
แผลเบาหวานเท้าครบ
วงจร (comprehensive
diabetic footcare
center)
รพ. สต. รพช.
(ขนาดเล็ก)
รพท., รพช.
(ขนาดใหญ่)
รพศ. รพ.มหาวิทยาลัย
บทบาท (ต่อ)
สั่งอุปกรณ์เสริมรองเท้า/รองเท้าพิเศษ ส่งต่อ ส่งต่อ ü ü ü
รักษาแผลระดับน้อย รักษาหรือ
ส่งต่อ
ü ü ü ü
รักษาแผลระดับปานกลาง ส่งต่อ รักษาหรือ
ส่งต่อ
ü ü ü
รักษาแผลระดับรุนแรง ส่งต่อ ส่งต่อ รักษาหรือส่งต่อ ü ü
ผ่าตัดรักษาเท้าผิดรูป ส่งต่อ ส่งต่อ ส่งต่อ รักษา
หรือ
ส่งต่อ
ü
ผ่าตัดรักษาโรคหลอดเลือดส่วน
ปลายตีบ
ส่งต่อ ส่งต่อ ส่งต่อ ส่งต่อ
ü
CPO: Certified Prosthetist Orthotist, CPed: Certified Pedorthist
8.2 การติดตามการด�ำเนินงานและการประเมินผลการดูแลภาวะแทรกซ้อนที่เท้าในผู้ป่วยเบาหวานของ
สถานพยาบาล
8.2.1 การติดตามและประเมินขั้นตอนการด�ำเนินงาน
การประเมินขั้นตอนการด�ำเนินงาน (process evaluation) ไม่ใช่การประเมินเพียงส่วนใด
ส่วนหนึ่งแต่หมายถึงการพิจารณาถึงองค์ประกอบหลายส่วนเข้าด้วยกันเช่นการด�ำเนินงานกิจกรรม
หน้าที่ ทรัพยากร เป็นต้น ตัวอย่างตัวชี้วัดในการประเมินขั้นตอนการด�ำเนินงาน ได้แก่
1) ร้อยละของผู้ป่วยเบาหวานที่ได้รับการตรวจเท้าอย่างละเอียดในช่วง 12 เดือนที่ผ่านมา
2) ร้อยละของผู้ป่วยเบาหวานที่ได้รับการประเมินระดับความเสี่ยงต่อการเกิดแผล
3) ร้อยละของผู้ป่วยเบาหวานที่มีความเสี่ยงปานกลางขึ้นไปที่ได้รับการดูแลโดยทีมสหสาขา
วิชาชีพในการดูแลเท้าเบาหวาน
ตารางที่ 8 บทบาทหน้าที่ของสถานพยาบาล (ต่อ)
36 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
เอกสารอ้างอิง
1. World HealthOrganization. World Health Statistics 2012 [internet]. Geniva: World
Health Organization; 2012 [cited 2012 Jun 12]. Available from: http://www.who.
int/gho/publications/world_health_statistics/2012/en/.
2. วิชัย เอกพลากร บรรณาธิการ. รายงานการส�ำรวจสุขภาพประชาชนไทยโดยการตรวจร่างกาย
ครั้งที่ 4 พ.ศ. 2551 -2. นนทบุรี: เดอะ กราฟิโก ซิสเต็มส์; 2553.
3. International Diabetes Federation. Diabetes fact sheet [internet]. Brussels:
International Working Group on the Diabetic Foot; 2005 [cited 2012 Jun 20].
Available from: http://www.idf.org/webdata/docs/background_info_AFR.pdf.
4. BartusCL,MargolisDJ.Reducingtheincidenceoffootulcerationandamputation
in diabetes. Curr Diab Rep. 2004 Dec;4(6):413-8.
5. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with
diabetes. JAMA. 2005 Jan 12;293(2):217-28.
6. Nitiyanant W, Chetthakul T, Sang AkP, Therakiatkumjorn C, Kunsuikmengrai K,
Yeo JP. A survey study on diabetes management and complication status in
primary care setting in Thailand. J Med Assoc Thai. 2007 Jan;90(1):65-71.
7. Rerkasem K. Seminar review: sociocultural practices and epidemiology of
diabetic foot problem: lessons from a study in Chiang Mai University
Hospital,Thailand. Int J Low Extrem Wounds. 2011 Jun;10(2):86-90.
8. Tantisiriwat N, Janchai S. Common foot problems in diabetic foot clinic. J Med
Assoc Thai. 2008 Jul;91(7):1097-101.
9. Rawdaree P, Ngarmukos C, Deerochanawong C, Suwanwalaikorn S, Chetthakul
T, Krittiyawong S, et al. Thailand diabetes registry (TDR) project: clinical status
and long term vascular complications in diabetic patients. J Med Assoc Thai.
2006 Aug;89 Suppl 1:S1-9.
38 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
56.
10. Gibson TB,Driver VR, Wrobel JS, Christina JR, Bagalman E, Defrancis R, et al.
Podiatristcareandoutcomesforpatientswithdiabetesandfootulcer.IntWound
J. 2013 Feb 4.
11. สถาบันวิจัยและประเมินเทคโนโลยีทางการแพทย์กรมการแพทย์,ส�ำนักงานหลักประกันสุขภาพ
แห่งชาติ.แนวทางเวชปฏิบัติการป้องกันดูแลรักษาภาวะแทรกซ้อนจากโรคเบาหวาน (ตาไตเท้า).
พิมพ์ครั้งที่ 2. กรุงเทพมหานคร: โรงพิมพ์ชุมนุมสหกรณ์การเกษตรแห่งประเทศไทย; 2553.
12. Krans HMJ, Porta M, Keen H, Staehr Johansen K, editors. Diabetes care and
researchinEurope:theStVincentdeclarationactionprogrammeimplementation
document. 2nd Ed. Copenhagen: World Health Organisation; 1995.
13. McIntosh A, Peters J, Young R, Hutchinson A, Chiverton R, Clarkson S, et al.
Prevention and management of foot problems in type 2 diabetes: clinical
guidelines and evidence. Sheffield: University of Sheffield; 2003.
14. Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of
diabetic foot disease. Lancet. 2005 Nov 12;366(9498):1719-24.
15. Walters DP, Gatling W, Mullee MA, Hill RD. The distribution and severity of
diabetic foot disease: a community study with comparison to a non-diabetic
group. Diabet Med. 1992 May;9(4):354-8.
16. Kumar S, Ashe HA, Parnell LN, Fernando DJ, Tsigos C, Young RJ, et al. The
prevalence of foot ulceration and its correlates in type 2 diabetic patients: a
population-based study. Diabet Med. 1994 Jun;11(5):480-4.
17. Neil HA, Thompson AV, Thorogood M, Fowler GH, Mann JI. Diabetes in the
elderly: the Oxford Community Diabetes Study. Diabet Med. 1989
Sep-Oct;6(7):608-13.
18. Moulik PK, Mtonga R, Gill GV. Amputation and mortality in new-onset diabetic
foot ulcers stratified by etiology. Diabetes Care. 2003 Feb;26(2):491-4.
39แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
57.
19. Potisat S,Krairittichai U, Jongsareejit A, Sattaputh C, Arunratanachote W. A 4-year
prospective study on long-term complications of type 2 diabetic patients: the
Thai DMS Diabetes Complications (DD.Comp.) project. J Med Assoc Thai. 2013;
96(6):637-43.
20. Thai Multicenter Research Group on Diabetes Mellitus. Vascular complications
in non-insulin dependent diabetics in Thailand. Diabetes Res Clin Pract. 1994
Aug;25(1):61-9.
21. Junrungsee S, Kosachunhanun N, Wongthanee A, Rerkasem K. History of foot
ulcers increases mortality among patients with diabetes in Northern Thailand.
Diabet Med. 2011 May;28(5):608-11.
22. Abbott CA, Carrington AL, Ashe H, Bath S, Every LC, Griffiths J, et al. The North-West
Diabetes Foot Care Study: incidence of, and risk factors for, new diabetic foot
ulcerationinacommunity-basedpatientcohort.DiabetMed.2002May;19(5):377-84.
23. Boyko EJ, Ahroni JH, Stensel V, Forsberg RC, Davignon DR, Smith DG. A prospective
study of risk factors for diabetic foot ulcer. The Seattle Diabetic Foot Study.
Diabetes Care. 1999 Jul;22(7):1036-42.
24. SriussadapornS,MekanandhaP,VannasaengS,NitiyanantW,KomoltriC,Ploybutr
S,etal.FactorsassociatedwithdiabeticfootulcerationinThailand:acase-control
study. Diabet Med. 1997 Jan;14(1):50-6.
25. Monteiro-Soares M,BoykoEJ,Ribeiro J,Ribeiro I,Dinis-Ribeiro M.Predictive factors
for diabetic foot ulceration: a systematic review. Diabetes Metab Res Rev. 2012
Oct;28(7):574-600.
26. Crawford F, Inkster M, Kleijnen J, Fahey T. Predicting foot ulcers in patients with
diabetes: a systematic review and meta-analysis. QJM. 2007 Feb;100(2):65-86.
27. MouraNetoA,Zantut-WittmannDE, FernandesTD,NeryM,ParisiMC.Riskfactors
for ulceration and amputation in diabetic foot: study in a cohort of 496 patients.
Endocrine. 2013 Aug;44(1):119-24.
40 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
58.
28. Valabhji J.Foot problems in patients with diabetes and chronic kidney disease.
J Ren Care. 2012 Feb;38 Suppl 1:99-108.
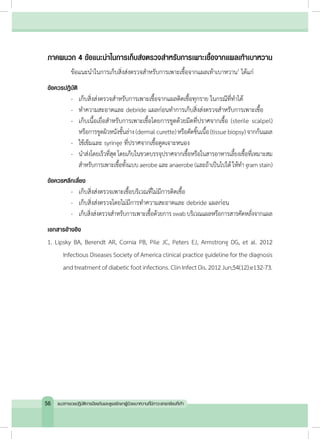
29. Lipsky BA, Berendt AR, Cornia PB, Pile JC, Peters EJ, Armstrong DG, et al. 2012
Infectious Diseases Society of America clinical practice guideline for the diagnosis
andtreatmentofdiabeticfootinfections.ClinInfectDis.2012Jun;54(12):e132-73.
30. Gupta AK, Konnikov N, MacDonald P, Rich P, Rodger NW, Edmonds MW, et al.
Prevalence and epidemiology of toenail onychomycosis in diabetic subjects:
a multicentre survey. Br J Dermatol. 1998 Oct;139(4):665-71.
31. Boyko EJ, Ahroni JH, Cohen V, Nelson KM, Heagerty PJ. Prediction of diabetic
foot ulcer occurrence using commonly available clinical information: the
Seattle Diabetic Foot Study. Diabetes Care. 2006 Jun;29(6):1202-7.
32. Winston JA, Miller JL. Treatment of onychomycosis in diabetic patients. Clin
Diabetes. 2006;24(4):160–6.
33. Welsh O, Vera-Cabrera L, Welsh E. Onychomycosis. Clin Dermatol. 2010 Mar
4;28(2):151-9.
34. Roberts DT, Taylor WD, Boyle J, British Association of D. Guidelines for treatment
of onychomycosis. Br J Dermatol. 2003 Mar;148(3):402-10.
35. Argoff CE, Backonja MM, Belgrade MJ, Bennett GJ, Clark MR, Cole BE, et al.
Diabetic peripheral neuropathic pain. Consensus guidelines for treatment. J Fam
Pract. 2006 Jun;Suppl:3-19.
36. Saarto T, Wiffen PJ. Antidepressants for neuropathic pain. Cochrane Database
Syst Rev. 2007 Oct 17;(4):CD005454.
37. Vinik A. Clinical review: use of antiepileptic drugs in the treatment of chronic
painful diabetic neuropathy. J Clin Endocrinol Metab. 2005 Aug;90(8):4936-45.
41แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
59.
38. Freeman R,Durso-Decruz E, Emir B. Efficacy, safety, and tolerability of pregabalin
treatment for painful diabetic peripheral neuropathy: findings from seven
randomized, controlled trials across a range of doses. Diabetes Care. 2008
Jul;31(7):1448-54.
39. Wiffen PJ, McQuay HJ, Edwards J, Moore RA. Withdrawn: Gabapentin for acute
and chronic pain. Cochrane Database Syst Rev. 2011 (3):CD005452.
40. Levin ME. Diabetes and peripheral neuropathy. Diabetes Care. 1998 Jan;21(1):1.
41. Younes NA, Ahmad AT. Diabetic foot disease. Endocr Pract. 2006
Sep-Oct;12(5):583-92.
42. Cofield RH, Morrison MJ, Beabout JW. Diabetic neuroarthropathy in the foot:
patient characteristics and patterns of radiographic change. Foot Ankle. 1983
Jul-Aug;4(1):15-22.
43. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural his-
tory of acute Charcot's arthropathy in a diabetic foot specialty clinic. J Am
Podiatr Med Assoc. 1997 Jun;87(6):272-8.
44. Apelqvist J, Bakker K, van Houtum WH, Schaper NC, International Working Group
on the Diabetic Foot Editorial B. Practical guidelines on the management and
prevention of the diabetic foot: based upon the International Consensus on the
Diabetic Foot (2007) Prepared by the International Working Group on the
Diabetic Foot. Diabetes Metab Res Rev. 2008 May-Jun;24 Suppl 1:S181-7.
45. Scottish Intercollegiate Guidelines Network. Management of diabetes a national
clinicalguideline[internet].Edinburgh:ScottishIntercollegiateGuidelinesNetwork;
2010 [cited 2012 Jun 12]. Available from: http://www.sign.ac.uk/pdf/sign116.pdf.
46. Boulton AJ, Kirsner RS, Vileikyte L. Clinical practice. Neuropathic diabetic foot
ulcers. N Engl J Med. 2004 Jul 1;351(1):48-55.
42 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
60.
47. SteedDL,Attinger C,ColaizziT,Crossland M,FranzM,Harkless L,etal.Guidelines
for the treatment of diabetic ulcers. Wound Repair Regen. 2006
Nov-Dec;14(6):680-92.
48. CavanaghPR,LipskyBA,BradburyAW,BotekG.Treatmentfordiabeticfootulcers.
Lancet. 2005 Nov 12;366(9498):1725-35.
49. The University of Michigan Medical School, The University of Michigan Health
System’s Educational Services for Nursing, Barry University School of Podiatric
Medicine. The standard of care for evaluation and treatment of diabetic foot
ulcers [Internet]. Michigan: Advanced BioHealing; 2010 [cited 2013 Feb 20].
Available from: https://www.barry.edu/includes/docs/continuing-medical-edu-
cation/diabetic.pdf.
50. Armstrong DG, Nguyen HC, Lavery LA, van Schie CH, Boulton AJ, Harkless LB.
Off-loading the diabetic foot wound: a randomized clinical trial. Diabetes Care.
2001 Jun;24(6):1019-22.
51. McIntosh C. Diabetic foot ulcers: what is best practice in the UK? Wound
Essentials [Internet]. 2007 [cited 2013 Feb 18];2:162-9. Available from: http://
www.wounds-uk.com/pdf/content_9405.pdf.
52. Bakker K, Apelqvist J, Schaper NC, International Working Group on Diabetic Foot
Editorial B. Practical guidelines on the management and prevention of the
diabetic foot 2011. Diabetes Metab Res Rev. 2012 Feb;28 Suppl 1:225-31.
53. Connor H, Mahdi OZ. Repetitive ulceration in neuropathic patients. Diabetes
Metab Res Rev. 2004 May-Jun;20 Suppl 1:S23-8.
54. Gadepalli R, Dhawan B, Sreenivas V, Kapil A, Ammini AC, Chaudhry R. A
clinico-microbiological study of diabetic foot ulcers in an Indian tertiary care
hospital. Diabetes Care. 2006 Aug;29(8):1727-32.
43แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
61.
55. Raymindo MFP,Mendoza MT. The microbiologic features and clinical outcome
of diabetic foot infections among patients admitted at UP-PGH. Phil J Microbiol
Infect Dis 2002;31(2):51-63.
56. Raja NS. Microbiology of diabetic foot infections in a teaching hospital in Malaysia:
a retrospective study of 194 cases. J Microbiol Immunol Infect. 2007 Feb;40(1):39-44.
57. American Diabetes Association. Consensus Development Conference on
Diabetic Foot Wound Care: 7-8 April 1999, Boston, Massachusetts. American
Diabetes Association. Diabetes Care. 1999 Aug;22(8):1354-60.
58. Dubsky M, Jirkovska A, Bem R, Fejfarova V, Skibova J, Schaper NC, et al. Risk
factors for recurrence of diabetic foot ulcers: prospective follow-up analysis of
a Eurodiale subgroup. Int Wound J. 2012 Jun 19.
59. Monami M, Longo R, Desideri CM, Masotti G, Marchionni N, Mannucci E. The
diabetic person beyond a foot ulcer: healing, recurrence, and depressive
symptoms. J Am Podiatr Med Assoc. 2008 Mar-Apr;98(2):130-6.
60. Lavery LA, Vela SA, Fleischli JG, Armstrong DG, Lavery DC. Reducing plantar
pressure in the neuropathic foot. A comparison of footwear. Diabetes Care. 1997
Nov;20(11):1706-10.
61. Lott DJ, Hastings MK, Commean PK, Smith KE, Mueller MJ. Effect of footwear
and orthotic devices on stress reduction and soft tissue strain of the
neuropathic foot. Clin Biomech (Bristol, Avon). 2007 Mar;22(3):352-9.
62. Burns J, Wegener C, Begg L, Vicaretti M, Fletcher J. Randomized trial of custom
orthoses and footwear on foot pain and plantar pressure in diabetic peripheral
arterial disease. Diabet Med. 2009 Sep;26(9):893-9.
63. Maland E, Walker C, Dalton J. Use of an EVA boot in a patient with a foot ulcer.
J Wound Care. 1997 Jul;6(7):319-20.
44 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
62.
64. Downs DM,Jacobs RL. Treatment of resistant ulcers on the plantar surface of
the great toe in diabetics. J Bone Joint Surg Am. 1982 Jul;64(6):930-3.
65. Holstein P, Larsen K, Sager P. Decompression with the aid of insoles in the
treatment of diabetic neuropathic ulcers. Acta Orthop Scand. 1976 Aug;47(4):463-8.
66. Larsen K, Fabrin J, Holstein PE. Incidence and management of ulcers in
diabetic Charcot feet. J Wound Care. 2001 Sep;10(8):323-8.
67. Chantelau E, Breuer U, Leisch AC, Tanudjaja T, Reuter M. Outpatient treatment
ofunilateraldiabeticfootulcerswith'halfshoes'.DiabetMed.1993Apr;10(3):267-70.
68. Reiber GE, Smith DG, Wallace C, Sullivan K, Hayes S, Vath C, et al. Effect of
therapeuticfootwearonfootreulcerationinpatientswithdiabetes:arandomized
controlled trial. JAMA. 2002 May 15;287(19):2552-8.
69. Viswanathan V, Madhavan S, Gnanasundaram S, Gopalakrishna G, Das BN,
Rajasekar S, et al. Effectiveness of different types of footwear insoles for the
diabetic neuropathic foot: a follow-up study. Diabetes Care. 2004 Feb;27(2):474-7.
70. UccioliL,FagliaE,MonticoneG,FavalesF,DurolaL,AldeghiA,etal.Manufactured
shoes in the prevention of diabetic foot ulcers. Diabetes Care. 1995 Oct;18(10):1376-8.
71. Mueller MJ, Strube MJ, Allen BT. Therapeutic footwear can reduce plantar
pressures in patients with diabetes and transmetatarsal amputation. Diabetes
Care. 1997 Apr;20(4):637-41.
72. Schaff PS, Cavanagh PR. Shoes for the insensitive foot: the effect of a "rocker
bottom" shoe modification on plantar pressure distribution. Foot Ankle. 1990
Dec;11(3):129-40.
73. Brown D, Wertsch JJ, Harris GF, Klein J, Janisse D. Effect of rocker soles on
plantar pressures. Arch Phys Med Rehabil. 2004 Jan;85(1):81-6.
74. Kastenbauer T, Sokol G, Auinger M, Irsigler K. Running shoes for relief of plantar
pressure in diabetic patients. Diabet Med. 1998 Jun;15(6):518-22.
45แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
63.
75. Praet SF,Louwerens JW. The influence of shoe design on plantar pressures in
neuropathic feet. Diabetes Care. 2003 Feb;26(2):441-5.
76. Brown JG. Medicare payments for therapeutic shoes. Philadelphia: Department
of Health and human services; 1998.
77. Harrison SJ, Cochrane L, Abboud RJ, Leese GP. Do patients with diabetes wear
shoes of the correct size? Int J Clin Pract. 2007 Nov;61(11):1900-4.
78. กุลภา ศรีสวัสดิ์, สุทิน ศรีอัษฎาพร. การดูแลรักษาและป้องกันแผลที่เท้าในผู้ป่วยเบาหวาน.
ใน: สุทิน ศรีอัษฎาพร, วรรณี นิธิยานันท์. โรคเบาหวาน. กรุงเทพฯ: เรือนแก้วการพิมพ์,
2548:583-608.
79. Lord M, Hosein R. Pressure redistribution by molded inserts in diabetic footwear:
a pilot study. J Rehabil Res Dev. 1994 Aug;31(3):214-21.
80. International Consensus on the Diabetic Foot and Practical and Specific
Guidelines on the Management and Prevention of the Diabetic Foot 2011.
International Working Group on the Diabetic Foot/Consultative Section of IDF.
81. ChantelauE,HaageP.Anauditofcushioneddiabeticfootwear:relationtopatient
compliance. Diabet Med. 1994 Jan-Feb;11(1):114-6.
82. KnowlesEA,BoultonAJ.Dopeoplewithdiabetesweartheirprescribedfootwear?
Diabet Med. 1996 Dec;13(12):1064-8.
83. Breuer U. Diabetic patient's compliance with bespoke footwear after healing of
neuropathic foot ulcers. Diabete Metab. 1994 Jul-Aug;20(4):415-9.
84. Williams AE, Nester CJ. Patient perceptions of stock footwear design features.
Prosthet Orthot Int. 2006 Apr;30(1):61-71.
46 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
เอกสารอ้างอิง
1. Pakarinen TK,Laine HJ, Honkonen SE, Peltonen J, Oksala H, Lahtela J. Charcot
arthropathy of the diabetic foot. Current concepts and review of 36 cases. Scand
J Surg. 2002;91(2):195-201.
2. Younes NA, Ahmad AT. Diabetic foot disease. Endocr Pract. 2006
Sep-Oct;12(5):583-92.
3. Qidwai SA,Khan MA,Hussain SR,Malik MS. Diabetic neuroarthropathy. Saudi Med
J. 2001 Feb;22(2):142-5.
4. Levin ME. Diabetes and peripheral neuropathy. Diabetes Care. 1998 Jan;21(1):1.
5. Edmonds ME.Thediabetic foot: pathophysiology and treatment. ClinEndocrinol
Metab. 1986 Nov;15(4):889-916.
6. Stevens MJ, Edmonds ME, Foster AV, Watkins PJ. Selective neuropathy and
preserved vascular responses in the diabetic Charcot foot. Diabetologia. 1992
Feb;35(2):148-54.
7. Green MF, Aliabadi Z, Green BT. Diabetic foot: evaluation and management.
South Med J. 2002 Jan;95(1):95-101.
8. Griffith J, Davies AM, Close CF, Nattrass M. Organized chaos? Computed
tomographic evaluation of the neuropathic diabetic foot. Br J Radiol. 1995
Jan;68(805):27-33.
9. LewDP,WaldvogelFA.Osteomyelitis.NEnglJMed.1997Apr3;336(14):999-1007.
10. Jaakkola J, Kehl D. Hematogenous calcaneal osteomyelitis in children. J Pediatr
Orthop. 1999 Nov-Dec;19(6):699-704.
11. Vázquez I, Moreno M, Larrosa M. Pamidronate treatment in Charcot
neuroosteoarthropathy: change in biochemical markers of bone turnover and
radiographic outcome after treatment. In: Harrison A , editor. Insights and Per-
52 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า
70.
spectives in Rheumatology.Rijeka: InTech; 2012 [cited 2013 Jun 12]. Available
from: http://www.intechopen.com/books/insights-and-perspectives-inrheuma-
tology/pamidronate-treatment-in-charcot-neuro-osteoarthropathy-change-in-
biochemical-markers-ofbone-turnov.
12. Sanders LJ, Frykberg RG. Charcot’s neuroarthropathy of the foot. In: Bowker JH,
Pfeifer MA, editors. Levin and O’Neal’s the diabetic foot. 6th ed. St Louis: CV
Mosby; 2001. p. 439-6.
13. Levin ME. Preventing amputation in the patient with diabetes. Diabetes Care.
1995 Oct;18(10):1383-94.
14. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural
history of acute Charcot's arthropathy in a diabetic foot specialty clinic. J Am
Podiatr Med Assoc. 1997 Jun;87(6):272-8.
15. Schon LC, Easley ME, Weinfeld SB. Charcot neuroarthropathy of the foot and
ankle. Clin Orthop Relat Res. 1998 Apr(349):116-31.
16. Pitocco D, Ruotolo V, Caputo S, Mancini L, Collina CM, Manto A, et al. Six-month
treatment with alendronate in acute Charcot neuroarthropathy: a randomized
controlled trial. Diabetes Care. 2005 May;28(5):1214-5.
17. Moreno M, Gratacos J, Casado E, Galisteo C, Orellana C, Larrosa M. [Usefulness
of Pamidronate in the Treatment of Charcot's Arthropathy]. Reumatol Clin. 2007
Nov;3(6):257-61.
18. Lee DK, Mulder GD. Stem cell applications in diabetic Charcot foot and ankle
reconstructive surgery. Wounds. 2010;22(9):226-9.
53แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า








































![เอกสารอ้างอิง
1. World Health Organization. World Health Statistics 2012 [internet]. Geniva: World
Health Organization; 2012 [cited 2012 Jun 12]. Available from: http://www.who.
int/gho/publications/world_health_statistics/2012/en/.
2. วิชัย เอกพลากร บรรณาธิการ. รายงานการส�ำรวจสุขภาพประชาชนไทยโดยการตรวจร่างกาย
ครั้งที่ 4 พ.ศ. 2551 -2. นนทบุรี: เดอะ กราฟิโก ซิสเต็มส์; 2553.
3. International Diabetes Federation. Diabetes fact sheet [internet]. Brussels:
International Working Group on the Diabetic Foot; 2005 [cited 2012 Jun 20].
Available from: http://www.idf.org/webdata/docs/background_info_AFR.pdf.
4. BartusCL,MargolisDJ.Reducingtheincidenceoffootulcerationandamputation
in diabetes. Curr Diab Rep. 2004 Dec;4(6):413-8.
5. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with
diabetes. JAMA. 2005 Jan 12;293(2):217-28.
6. Nitiyanant W, Chetthakul T, Sang AkP, Therakiatkumjorn C, Kunsuikmengrai K,
Yeo JP. A survey study on diabetes management and complication status in
primary care setting in Thailand. J Med Assoc Thai. 2007 Jan;90(1):65-71.
7. Rerkasem K. Seminar review: sociocultural practices and epidemiology of
diabetic foot problem: lessons from a study in Chiang Mai University
Hospital,Thailand. Int J Low Extrem Wounds. 2011 Jun;10(2):86-90.
8. Tantisiriwat N, Janchai S. Common foot problems in diabetic foot clinic. J Med
Assoc Thai. 2008 Jul;91(7):1097-101.
9. Rawdaree P, Ngarmukos C, Deerochanawong C, Suwanwalaikorn S, Chetthakul
T, Krittiyawong S, et al. Thailand diabetes registry (TDR) project: clinical status
and long term vascular complications in diabetic patients. J Med Assoc Thai.
2006 Aug;89 Suppl 1:S1-9.
38 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า](https://image.slidesharecdn.com/2556-131010202831-phpapp02/85/2556-55-320.jpg)
![38. Freeman R, Durso-Decruz E, Emir B. Efficacy, safety, and tolerability of pregabalin
treatment for painful diabetic peripheral neuropathy: findings from seven
randomized, controlled trials across a range of doses. Diabetes Care. 2008
Jul;31(7):1448-54.
39. Wiffen PJ, McQuay HJ, Edwards J, Moore RA. Withdrawn: Gabapentin for acute
and chronic pain. Cochrane Database Syst Rev. 2011 (3):CD005452.
40. Levin ME. Diabetes and peripheral neuropathy. Diabetes Care. 1998 Jan;21(1):1.
41. Younes NA, Ahmad AT. Diabetic foot disease. Endocr Pract. 2006
Sep-Oct;12(5):583-92.
42. Cofield RH, Morrison MJ, Beabout JW. Diabetic neuroarthropathy in the foot:
patient characteristics and patterns of radiographic change. Foot Ankle. 1983
Jul-Aug;4(1):15-22.
43. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural his-
tory of acute Charcot's arthropathy in a diabetic foot specialty clinic. J Am
Podiatr Med Assoc. 1997 Jun;87(6):272-8.
44. Apelqvist J, Bakker K, van Houtum WH, Schaper NC, International Working Group
on the Diabetic Foot Editorial B. Practical guidelines on the management and
prevention of the diabetic foot: based upon the International Consensus on the
Diabetic Foot (2007) Prepared by the International Working Group on the
Diabetic Foot. Diabetes Metab Res Rev. 2008 May-Jun;24 Suppl 1:S181-7.
45. Scottish Intercollegiate Guidelines Network. Management of diabetes a national
clinicalguideline[internet].Edinburgh:ScottishIntercollegiateGuidelinesNetwork;
2010 [cited 2012 Jun 12]. Available from: http://www.sign.ac.uk/pdf/sign116.pdf.
46. Boulton AJ, Kirsner RS, Vileikyte L. Clinical practice. Neuropathic diabetic foot
ulcers. N Engl J Med. 2004 Jul 1;351(1):48-55.
42 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า](https://image.slidesharecdn.com/2556-131010202831-phpapp02/85/2556-59-320.jpg)
![47. SteedDL,Attinger C,Colaizzi T,Crossland M,FranzM,Harkless L,etal.Guidelines
for the treatment of diabetic ulcers. Wound Repair Regen. 2006
Nov-Dec;14(6):680-92.
48. CavanaghPR,LipskyBA,BradburyAW,BotekG.Treatmentfordiabeticfootulcers.
Lancet. 2005 Nov 12;366(9498):1725-35.
49. The University of Michigan Medical School, The University of Michigan Health
System’s Educational Services for Nursing, Barry University School of Podiatric
Medicine. The standard of care for evaluation and treatment of diabetic foot
ulcers [Internet]. Michigan: Advanced BioHealing; 2010 [cited 2013 Feb 20].
Available from: https://www.barry.edu/includes/docs/continuing-medical-edu-
cation/diabetic.pdf.
50. Armstrong DG, Nguyen HC, Lavery LA, van Schie CH, Boulton AJ, Harkless LB.
Off-loading the diabetic foot wound: a randomized clinical trial. Diabetes Care.
2001 Jun;24(6):1019-22.
51. McIntosh C. Diabetic foot ulcers: what is best practice in the UK? Wound
Essentials [Internet]. 2007 [cited 2013 Feb 18];2:162-9. Available from: http://
www.wounds-uk.com/pdf/content_9405.pdf.
52. Bakker K, Apelqvist J, Schaper NC, International Working Group on Diabetic Foot
Editorial B. Practical guidelines on the management and prevention of the
diabetic foot 2011. Diabetes Metab Res Rev. 2012 Feb;28 Suppl 1:225-31.
53. Connor H, Mahdi OZ. Repetitive ulceration in neuropathic patients. Diabetes
Metab Res Rev. 2004 May-Jun;20 Suppl 1:S23-8.
54. Gadepalli R, Dhawan B, Sreenivas V, Kapil A, Ammini AC, Chaudhry R. A
clinico-microbiological study of diabetic foot ulcers in an Indian tertiary care
hospital. Diabetes Care. 2006 Aug;29(8):1727-32.
43แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า](https://image.slidesharecdn.com/2556-131010202831-phpapp02/85/2556-60-320.jpg)






![spectives in Rheumatology. Rijeka: InTech; 2012 [cited 2013 Jun 12]. Available
from: http://www.intechopen.com/books/insights-and-perspectives-inrheuma-
tology/pamidronate-treatment-in-charcot-neuro-osteoarthropathy-change-in-
biochemical-markers-ofbone-turnov.
12. Sanders LJ, Frykberg RG. Charcot’s neuroarthropathy of the foot. In: Bowker JH,
Pfeifer MA, editors. Levin and O’Neal’s the diabetic foot. 6th ed. St Louis: CV
Mosby; 2001. p. 439-6.
13. Levin ME. Preventing amputation in the patient with diabetes. Diabetes Care.
1995 Oct;18(10):1383-94.
14. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural
history of acute Charcot's arthropathy in a diabetic foot specialty clinic. J Am
Podiatr Med Assoc. 1997 Jun;87(6):272-8.
15. Schon LC, Easley ME, Weinfeld SB. Charcot neuroarthropathy of the foot and
ankle. Clin Orthop Relat Res. 1998 Apr(349):116-31.
16. Pitocco D, Ruotolo V, Caputo S, Mancini L, Collina CM, Manto A, et al. Six-month
treatment with alendronate in acute Charcot neuroarthropathy: a randomized
controlled trial. Diabetes Care. 2005 May;28(5):1214-5.
17. Moreno M, Gratacos J, Casado E, Galisteo C, Orellana C, Larrosa M. [Usefulness
of Pamidronate in the Treatment of Charcot's Arthropathy]. Reumatol Clin. 2007
Nov;3(6):257-61.
18. Lee DK, Mulder GD. Stem cell applications in diabetic Charcot foot and ankle
reconstructive surgery. Wounds. 2010;22(9):226-9.
53แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า](https://image.slidesharecdn.com/2556-131010202831-phpapp02/85/2556-70-320.jpg)
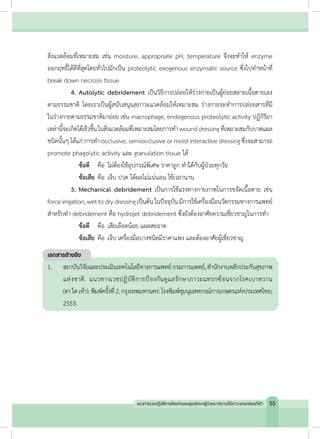





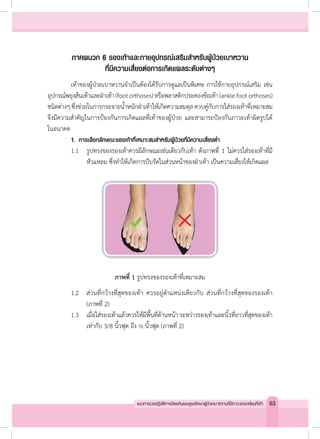


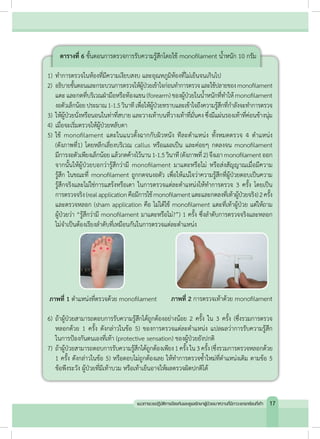
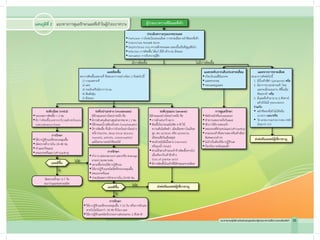
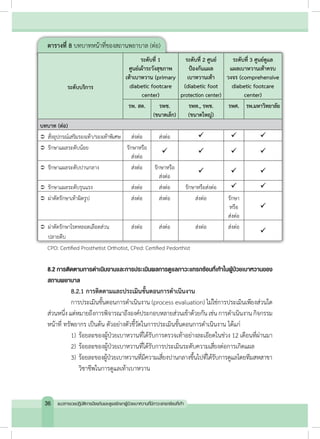
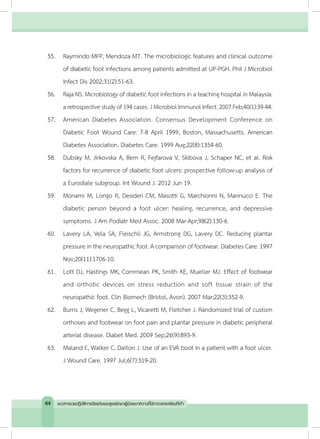
![ภาพที่ 6 ตัวอย่างรองเท้าส�ำหรับใส่เดินภายในบ้าน
3. ลักษณะรองเท้าและกายอุปกรณ์เสริมที่เหมาะสมส�ำหรับผู้ป่วยที่มีความเสี่ยงสูง
กรณีที่ผู้ป่วยมีเท้าผิดรูป พิจารณาอุปกรณ์พยุงส้นเท้าและฝ่าเท้าเพิ่มเติมหรือพลาสติก
ดามข้อเท้า (ankle foot orthoses) ดังภาพที่ 71
เพื่อลดแรงกดทับในจุดที่มีความผิดปกติไปให้เท้า
ทุกส่วนได้รับความสมดุลมากที่สุด ควบคู่กับรองเท้าที่เหมาะสมส�ำหรับความผิดปกตินั้นๆ (ภาพที่ 8)
ภาพที่ 7 ตัวอย่างพลาสติกดามข้อเท้า ภาพที่ 8 ตัวอย่างรองเท้าที่เหมาะสม
1. Fidelity Orthopedic. Information for health care professionals. [cited 2013 May
21]. Available from: http://www.fidelityorthopedic.com/orthodicproducts.html.
เอกสารอ้างอิง
66 แนวทางเวชปฏิบัติการป้องกันและดูแลรักษาผู้ป่วยเบาหวานที่มีภาวะแทรกซ้อนที่เท้า](https://image.slidesharecdn.com/2556-131010202831-phpapp02/85/2556-83-320.jpg)