23204931
•
5 likes•1,803 views

The document describes a case of a 3-week-old infant referred for tachypnea. Chest x-ray showed cardiomegaly and normal pulmonary vascularity. Aortogram showed normal aorta but retrograde filling of the left coronary artery from collaterals, with the proximal left coronary draining into the pulmonary artery rather than the aorta. The most likely diagnosis is Bland-White-Garland Syndrome, a rare condition where one coronary artery, usually the left, originates from the pulmonary artery rather than the aorta.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to 23204931
Similar to 23204931 (20)
More from radgirl
Recently uploaded
Recently uploaded (20)
23204931
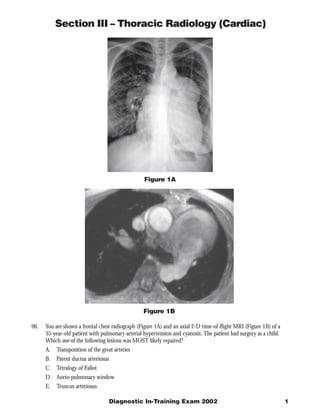
- 1. Section III – Thoracic Radiology (Cardiac) Figure 1A Figure 1B 96. You are shown a frontal chest radiograph (Figure 1A) and an axial 2-D time-of-flight MRI (Figure 1B) of a 35-year-old patient with pulmonary arterial hypertension and cyanosis. The patient had surgery as a child. Which one of the following lesions was MOST likely repaired? A. Transposition of the great arteries B. Patent ductus arteriosus C. Tetralogy of Fallot D. Aorto-pulmonary window E. Truncus arteriosus Diagnostic In-Training Exam 2002 1
- 2. Section III – Thoracic Radiology (Cardiac) Question #96 Findings: The radiograph demonstrates enlarged central pulmonary arteries compatible with pulmonary arterial hypertension. The central pulmonary arteries also have calcified walls. In addition, there is deformity of the left upper ribs compatible with a prior thoracotomy. The MR confirms the presence of enlarged central pulmonary arteries and decreased signal in the central branches suggesting slow flow from elevated resistance. There is also an anastomosis between the left pulmonary artery and the descending aorta. Rationales: A) Incorrect. Repair of D-transposition of the Great Arteries usually takes place through a median sternotomy not a posterior thoracotomy as this case. Transposition repair can be done by an atrial switch operation (Mustard, Senning) in which the systemic venous and pulmonary venous blood are re-routed appropriately, and more recently by the arterial switch or Jatene operation in which the great arteries themselves are relocated to their respective ventricles. The surgical connection between the descending aorta and pulmonary artery in the test case cannot be explained on the basis of any of these operations, therefore excluding transposition as an option. B) Incorrect. Repair of a patent ductus arteriosus requires ligation of the ductus. This is done through a left thoracotomy. An anastomosis between the pulmonary artery and aorta is not required. Moreover, pulmonary hypertension is not expected after surgical repair. Thus, although the rib changes can be seen after PDA repair, the pulmonary artery to aorta conduit is not consistent with this type of repair. C) Correct. Surgical palliation of TOF usually requires anastomosis between the obstructed right heart and systemic circulation before definitive repair is performed. The Potts-Smith operation was performed in this patient. In this palliative operation, the descending aorta and left pulmonary artery are anastomosed in a side- by-side fashion through a thoracotomy. Unfortunately, a common complication of this procedure is the development of pulmonary arterial hypertension because of increased blood flow to the lungs if the size of the anastomosis is not carefully constructed. The findings of pulmonary hypertension, a left thoracotomy and the surgical anastomosis between the systemic and pulmonary circulations support the diagnosis of tetralogy of Fallot. More recently, definitive repair of tetralogy of Fallot is performed early in life when feasible, thus obviating temporizing palliating procedures. The Potts-Smith operation has essentially been abandoned. D) Incorrect. An aorto-pulmonary window is a congenital defect in which there is a broad-based connection between the proximal aorta and the pulmonary artery. This condition can result in pulmonary artery hypertension if surgical repair is not done. However, the increased pulmonary flow characteristic of this anomaly prior to surgery usually regresses completely or nearly so after surgery. Repair requires closing the abnormal communication generally through an sternal splitting anterior approach. In the test patient, the left posterior thoracotomy as well as the anastomosis between the descending aorta and pulmonary artery argue against the diagnosis of aorto-pulmonary window. E) Incorrect. Prior to surgical repair, the shunt in truncus arteriosus is at the level of the ascending aorta and pulmonary artery. Repair requires separation of the pulmonary arteries from the aortic segment and then reconnection to the right ventricle, usually with an aortic homograft conduit. The conduit may eventually calcify. Normal vascularity is expected after surgery. In the test patient, the pulmonary hypertension and the shunt at the level of the descending, rather than the ascending, aorta make truncus arteriosus untenable. In addition, surgical repair of truncus is performed through a sternal splitting anterior approach, not through a thoracotomy. Citations: Potts WJ, Smith S, Gibson S. Anastomosis of the aorta to a pulmonary artery. JAMA 132:627, 1946 Piccoli GP, Dickinson DF, Musumeci F, Hamilton DI. A changing policy for the surgical treatment of tetralogy of Fallot: Early and late results in 235 consecutive patients. Ann Thorac Surg 33:365, 1982 RL Soulen, RM Donner, and M Capitanio. Postoperative evaluation of complex congenital heart disease by magnetic resonance imaging. RadioGraphics 1987 7: 975-1000 2 American College of Radiology
- 3. Section III – Thoracic Radiology (Cardiac) Figure 2A Figure 2B 97. You are shown a plain radiograph (Figure 2A) and a right ventriculogram (Figure 2B) of a 2-day-old infant with tachypnea and cyanosis. Which one of the following is the MOST likely diagnosis? A. Tetralogy of Fallot B. Truncus arteriosus C. Pulmonary atresia and intact ventricular septum D. Ebstein’s anomaly of tricuspid valve E. D-transpostion of the great vessels Diagnostic In-Training Exam 2002 3
- 4. Section III – Thoracic Radiology (Cardiac) Question #97 Findings: The chest radiograph demonstrates decreased pulmonary vascularity with a normal heart size and slight elevation of the cardiac apex. The location of the aortic arch is not readily visible on this radiograph. The right ventriculogram reveals opacification of the aorta, indicating a ventricular septal defect shunting right-to-left and hypoplasia of the right ventricular outflow tract. Other findings include competent tricuspid and mitral valves. The findings are consistent with Tetralogy of Fallot. Rationales: A. Correct. Tetralogy of Fallot is the most common cardiac cause of neonatal cyanosis. Anatomic features of Tetralogy of Fallot include a VSD, pulmonic stenosis, overriding aorta, and right ventricular hypertrophy. If there is severe obstruction of the right ventricular outflow tract, right to left shunting occurs across the VSD. Infants with severe obstruction usually present soon after birth with cyanosis and dyspnea. The infundibular stenosis results in decreased pulmonary vascularity on chest radiographs. The cardiac size is normal with an uplifted apex as a result of the right ventricular hypertrophy. The right heart obstruction, concomitant hypoplasia of the right ventricular outflow tract and atretic pulmonary valve in this patient is characteristic of severe tetralogy of Fallot also known as pseudotruncus arteriosus. B. Incorrect. Truncus arteriosus is a cyanotic cardiac anomaly characterized by a single arterial trunk arising from the heart and giving origin to the pulmonary arteries and ascending aorta. There is a single truncal valve which may have 3 to 6 semilunar leaflets. Invariably, there is a large VSD below the valve leaflets. Pulmonary vascularity is markedly increased because blood flows from the aorta to the pulmonary circulation. The cardiac size is enlarged. The decreased pulmonary vascularity, normal heart size and 2 separate semilunar valves demonstrated on the ventriculogram essentially exclude the diagnosis of truncus. C. Incorrect. In patients with pulmonary atresia and intact ventricular septum (also referred to as trilogy of Fallot) there is no communication between the pulmonary outflow tract and the right ventricle. The right ventricle is usually hypoplastic. There is also obligatory right to left shunting across an atrial septal defect. The absence of antegrade flow through the pulmonary valve results in diminished pulmonary vascularity on chest radiography. The heart is usually normal size in the immediate postnatal period. The chest radiographic findings in the test patient are compatible with pulmonary atresia and intact ventricular septum. However, the presence of a ventricular septal defect on the right ventriculogram excludes the diagnosis. D. Incorrect. Patients with Ebstein’s anomaly have a redundant tricuspid valve which is adherent to the right ventricular wall distal to the annulus of the tricuspid valve. This results in tricuspid regurgitation and subsequent right atrial enlargement. The right ventricle is decreased in size and is slow to empty, leading to decreased blood flow into the pulmonary arteries and right to left shunting across a patent foramen ovale or atrial septal defect. Hence, affected infants are usually cyanotic. The combination of decreased vascularity, a normal heart size and a competent tricuspid valve on the ventriculogram in the test patient makes Ebstein anomaly an unlikely diagnosis. E. Incorrect. D transposition of the great vessels (TGV) occurs when the aorta and main pulmonary artery arise from the morphologic right ventricle and morphologic left ventricle, respectively, creating two circulations in parallel. Desaturated venous blood flows from the right atrium into the right ventricle and then into the aorta, resulting in cyanosis. Radiographic findings include a narrow mediastinum, mild cardiomegaly and prominent pulmonary vascularity. The normal heart size and decreased vascularity in the test case would be unusual in a patient with d-TGV. Citations: Van Praagh R, Van Praagh S, Nebesar RA et al: Tetralogy of Fallot. Underdevelopment of the pulmonary infundibulum and its sequelae. Am J Cardiol 26:25-33, 1970 Adams FH, Emmanoulides GC, Riemenschneider TA. In Heart Disease in Infants, Children, and Adolescents. Fourth Edition Williams, Wilkins Baltimore 1989 4 American College of Radiology
- 5. Section III – Thoracic Radiology (Cardiac) Figure 3A Figure 3B 98. This 63-year-old patient presented with chest pain. You are shown two levels (Figure 3A and Figure 3B) of a contrast enhanced CT scan. Which one of the following is the MOST likely diagnosis? A. Arrhythmogenic right ventricular dysplasia B. Congenital partial absence of the pericardium C. Left ventricular aneurysm D. Pericardial cyst E. Sinus of Valsalva aneurysm Diagnostic In-Training Exam 2002 5
- 6. Section III – Thoracic Radiology (Cardiac) Question #98 Findings: The CT scan demonstrates a large mass that fills part of the anterior mediastinum in front of the pulmonary outflow tract (A). This mass contains calcification. Image (B) obtained at a lower level shows that the mass is in continuity with the left ventricle. In addition, the left ventricular wall is thin in the anteroseptal portion with subendocardial mural thrombus formation and peripheral calcification. All of these findings in combination are diagnostic of a large left ventricular aneurysm that extends superiorly into the anterior mediastinum Rationales: A. Incorrect. Arrhythmogenic right ventricular dysplasia is a condition in which fibrofatty replacement of the ventricular wall can lead to outpouchings in the wall of the right ventricle. Patients have frequent ventricular arrhythmias, and sudden death has been described. A large calcified mass as seen in this case would be atypical. In addition, the mass in the test patient arises from the left ventricle and the right ventricle appears normal, thus excluding such a diagnosis. B. Incorrect. Congenital absence of the pericardium can be total or partial. The partial form is the most common, usually involving the portion of the pericardium along the left heart border near the left atrial appendage. Patients can present clinically with chest pain, and strangulation of the left atrial appendage has been described. CT shows a protrusion of the left ventricle through the area of absent pericardium. The thickness of the ventricular wall is normal. The findings in the test patient of a thinned ventricular wall and a calcified mass in continuity with the anterior left ventricular wall excludes absence of the pericardium as a diagnostic alternative. C. Correct. There is thinning of the left ventricular wall over its entire anteroseptal aspect. Mural thrombus is seen on the inside of the thin ventricular wall. In addition, a large aneurysm has formed which has extended superiorly in front of the right ventricular outflow tract. This aneurysm has partly calcified over time. The findings are diagnostic of a left ventricular aneurysm. D. Incorrect. Pericardial cyst is a congenital entity related to the celomic cavity, in which a fluid containing structure forms adjacent to and not in communication with the pericardial cavity. Most are located in the right cardiophrenic angle. Heart chambers are not involved in the condition. The typical CT findings of pericardial cyst are those of a water attenuation mass adjacent to the cardiac border. A soft tissue attenuation mass with areas of calcification and the left ventricular involvement shown in the test case exclude a pericardial cyst. E. Incorrect. Sinus of Valsalva aneurysm results from a deficiency between the aortic media and fibrous annulus of the aortic valve resulting in distension and eventual aneurysm formation. If the aneurysm becomes large enough, it can rupture into the right atrial or right ventricular cavity. The test case demonstrates predominantly a left ventricular process excluding this diagnosis of sinus of Valsalva aneurysm. Citations: Adams FH, Emmanoulides GC, Riemenschneider TA. In Heart Disease in Infants, Children, and Adolescents. Fourth Edition Williams, Wilkins Baltimore 1989 Dahnert Wolfgang. Radiology Review Manual. Lippincott Williams and Wilkins 4th Edition 1999 6 American College of Radiology
- 7. Section III – Thoracic Radiology (Cardiac) Figure 4A Figure 4B 99. An afebrile 3-week-old infant is referred because of tachypnea. A chest radiograph (Figure 4A) was obtained. This was followed by an electrocardiogram, which was abnormal, as well as an aortogram (Figure 4B). Which one of the following is the MOST likely diagnosis? A. Hypoplastic left heart syndrome B. Bland-White-Garland syndrome C. Kawasaki arteritis D. Single coronary artery E. Aortic insufficiency Diagnostic In-Training Exam 2002 7
- 8. Section III – Thoracic Radiology (Cardiac) Question #99 Findings: The frontal chest radiograph shows cardiomegaly, normal pulmonary vascularity and retrocardiac atelectasis. A left sided obstructive lesion should be suspected. Aortogram shows a normal aortic valve and ascending aorta. However, the left coronary artery fills in a retrograde fashion by collaterals from the right coronary artery. No connection is seen between the proximal left coronary system and the aorta. On the other hand, it appears that the proximal left coronary artery drains to the region of the main pulmonary artery. Also note that the left anterior descending and circumflex branches come together as a common trunk. Rationales: A. Incorrect. The term hypoplastic left heart syndrome refers to a spectrum of anomalies characterized by a poorly developed left ventricle and ascending aorta. There is often underdevelopment of the mitral valve and left atrium. The resultant pathology is that there is no forward flow of blood from the left ventricle and so congestive heart failure is common soon after birth. Chest radiographs usually demonstrate cardiomegaly, increased vascularity and pulmonary edema. The normal pulmonary vascularity in the test radiographs and normal size aortic valve and ascending aorta on the aortogram make hypoplastic left heart unlikely. B. Correct. Bland-White –Garland Syndrome is a rare condition in which one of the coronary arteries (usually the left) originates from the pulmonary artery. Shortly after birth as the pulmonary artery resistance normally decreases, the myocardial perfusion from the anomalous coronary is compromised, resulting in ischemia and transmural infarction Patients present with congestive heart failure as a result of the ischemic insult. ECG usually suggests the diagnosis. C. Incorrect. Kawasaki arteritis is an acute febrile vasculitis of childhood. The illness occurs in young children, approximately 80% are under 5 years of age. Rarely, it affects infants or adolescents. Kawasaki disease causes a severe vasculitis of all blood vessels, with predilection for the coronary arteries. Acutely, patients present with high spiking fevers. Cardiomegaly and normal vascularity can be seen on chest radiographs. Aneurysms of the coronary arteries are common, but anomalous coronary origin is not a feature of this disease. The age of the test patient and the abnormal coronary artery anatomy makes Kawasaki disease unlikely. D. Incorrect. Rarely, infants are born with a single coronary artery. Most often, there is a single left branch which courses between the aorta and pulmonary artery . The anomalous artery can be “pinched” between the two vessels, resulting in ischemia and sudden death. In the test patient, there are two coronary arteries, excluding the diagnosis of a single artery. E. Incorrect. In the test patient, the left anterior descending (LAD) branch of the coronary artery and the circumflex branch join together as a common trunk, thus excluding the diagnosis of an anomalous origin. Anomalous origin of the LAD is particularly common in patients with tetralogy of Fallot, occurring in 5 to 9% of this population This anatomic variant can have important surgical implications at total repair. Citation: Choh JH, Levinsky L, Srinivasan V, Idbeis B, Subramanian S. Anomalous origin of the left coronary artery from the pulmonary trunk: Its clinical spectrum and current surgical management. Thorac and Cardiovasc Surg 28:239-242, 1980. 8 American College of Radiology
- 9. Section III – Thoracic Radiology (Cardiac) Figure 5A Figure 5B 100. You are shown an axial T1-weighted turbo spin-echo (Figure 5A) and coronal gradient echo image (Figure 5B) of a 13-year-old girl with a diastolic murmur in the left precordial space. Which one of the following is the MOST likely diagnosis? A. Rheumatic aortic valvular disease B. Bicuspid aortic valve C. Aortic dissection D. Williams syndrome E. Takayasu’s arteritis Diagnostic In-Training Exam 2002 9
- 10. Section III – Thoracic Radiology (Cardiac) Question #100 (question was not scored in the exam) Both sequences demonstrate an enlarged aortic root that measures approximately 4.5 cm in diameter. In addition, there is thickening of the walls of the ascending aorta and pulmonary arteries. The gradient echo image demonstrates a mild degree of aortic valvular insufficiency. The findings are consistent with an arteritis, such as Takayasu’s arteritis. Rationales: A. Incorrect. Rheumatic fever is an inflammatory condition that affects primarily the heart. The inflammatory process can involve the heart valves producing scarring that can lead to stenosis as well as insufficiency. The walls of the great vessels are not affected by the condition, thus excluding the diagnosis in the test case. B. Incorrect. Bicuspid aortic valve is a common congenital defect affecting the aortic valve, occurring in 1-2% of the population. Due to hemodynamic alteration of the flow through the valve, fibrosis and eventual calcification ensue producing stenosis. Although the enlargement of the aortic root from post-stenotic dilatation as well as the mild degree of valvular regurgitation could be explained on the basis of a bicuspid aortic valve, the thickening of the aortic and pulmonary arteries excludes the diagnosis. C. Incorrect. Aortic dissection is associated with an intramural hematoma which produces widening of the aorta. True wall thickening does not occur. A late sequela can be aortic insufficiency. Although the finding of aortic valvular insufficiency in the test case is consistent with dissection, the presence of wall thickening is atypical for dissection. Moreover, the patient’s age is unusual for this diagnosis. D. Incorrect. Williams syndrome is an autosomal dominant condition that is characterized by aortitis, mental retardation and elfin-like facies. Although thickening of the wall of the ascending aorta and pulmonary artery can be a feature of the disease, there is usually narrowing of the lumen of the ascending aorta causing supravalvular stenosis that can be diffuse at times. The aortic root dilatation seen in the test case virtually excludes Williams syndrome. E. Correct. Takayasu arteritis is a granulomatous inflammation of the aorta, its branches and the pulmonary artery. It usually affects persons younger than 50 years of age. An acute stage that is characterized by a granulomatous infiltrate of elastic fibers of media of arterial walls is followed by a chronic fibrotic period that eventually leads to fibrosis of the media and adventitia. Takayasu arteritis is divided into several types. Type IV is the so called dilated type, which affects aorta and its branches as well as the pulmonary arteries. Citations: Danhert Wolfgang in Radiology Review Manual 4th Edition Lippincott-Williams Wilkins 1999 10 American College of Radiology