Downloaded 194 times

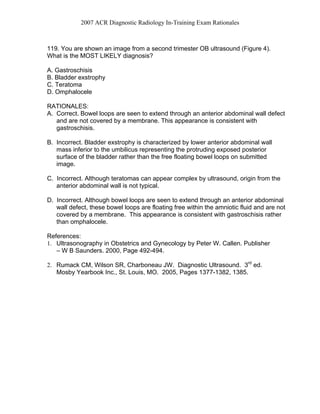
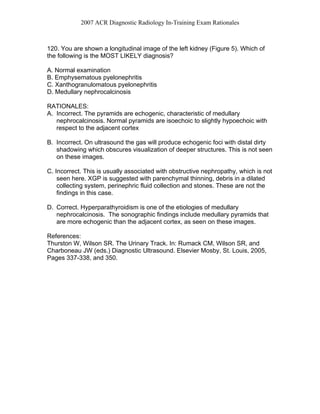
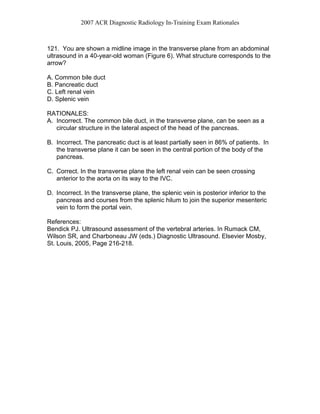





This document provides rationales for questions from the 2007 ACR Diagnostic Radiology In-Training Exam related to ultrasound imaging. It discusses the correct answers and rationales for questions regarding various pathologies seen on ultrasound of the uterus, testes, kidneys, abdomen and fetal anatomy. Key details include identifying a cornual pregnancy based on its location, tubular ectasia of the rete testis in an older male, medullary nephrocalcinosis seen as echogenic renal pyramids, the left renal vein in the transverse abdominal image, and measuring fetal head circumference at the level of the thalami and cavum septi pellucidi.