
Download to read offline

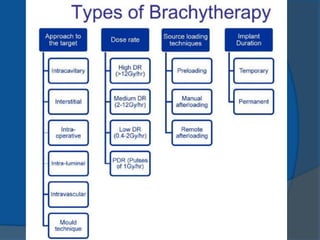


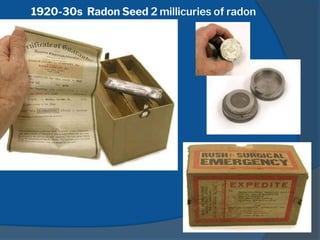
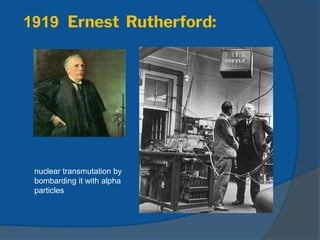
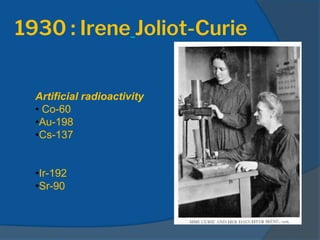
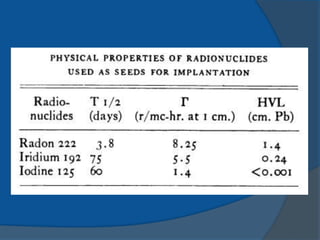
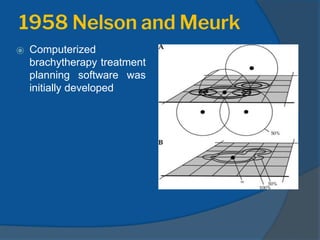
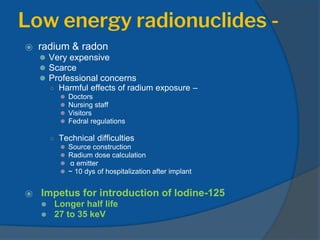
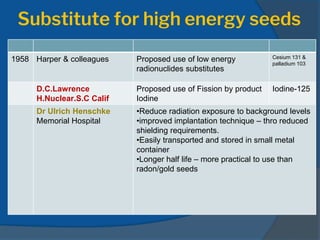

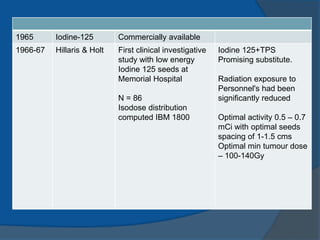

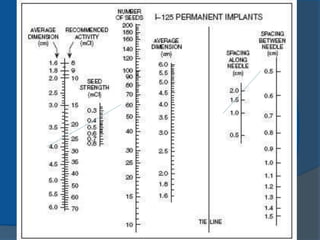
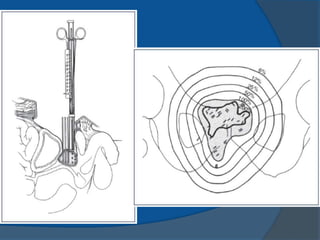
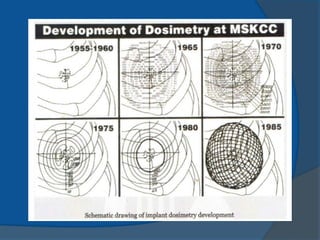
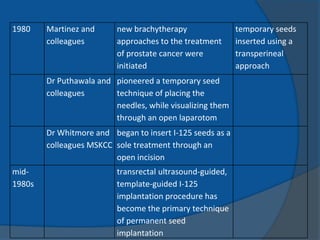
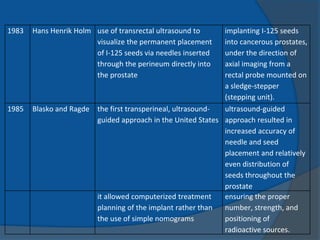












This document provides an introduction to permanent implant brachytherapy. It discusses the history and origins of brachytherapy techniques from the late 19th century discoveries of radioactivity through modern developments. Key events include the first radium implants in the early 1900s, introduction of iodine-125 seeds in the 1960s as a safer alternative to radium, and the development of ultrasound-guided seed implantation in the 1980s. Transrectal ultrasound guidance has allowed for improved accuracy and distribution of seeds compared to earlier techniques. Permanent brachytherapy seed implantation is now commonly used to treat prostate cancer.























































































