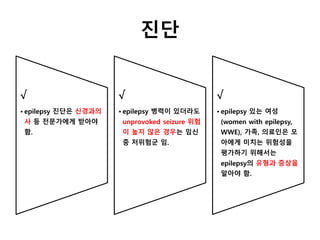
진단
√
• epilepsy 진단은신경과의
사 등 전문가에게 받아야
함.
√
• epilepsy 병력이 있더라도
unprovoked seizure 위험
이 높지 않은 경우는 임신
중 저위험군 임.
√
• epilepsy 있는 여성
(women with epilepsy,
WWE), 가족, 의료인은 모
아에게 미치는 위험성을
평가하기 위해서는
epilepsy의 유형과 증상을
알아야 함.
감별 진단
√
• 임신후반기에 seizure 있는데
epilepsy로 인한 것인지 명확하지
않은 경우 신경과적 평가가 완전히
이루어지기전까지는 eclampsia 치
료 프로토콜을 따라야 함.
√
• 다른 심장, 대사성, 대뇌 질환도 감
별 진단으로 고려해야 함. 비간질성
발작 질환과 같은 신경정신과적 상
태도 고려되어야 함.
6.
항전간제의 위험
√
•임신 계획중인 WWE은 태아에 위험성과 발작의 조절 모두를 고려하여 항전간제(antiepileptic drugs,
AEDs) 종류와 용량을 결정할 주치의가 있어야 함.
C
•WWE에게 수태기에 AEDs에 노출되지 않았다면 대부분 정상적이고 건강한 아기를 가지고 선천성 기
형 위험은 낮다는 것을 알려 안심시켜야 함.
B
•임신부에게 태아에게 미치는 선천성 기형 위험은 AEDs의 종류, 수, 용량에 따라 다르다는 것을 알려야 함.
7.
장기 신경발달학적 결과
C
•WWE와 배우자에게 sodium valproate 약물 복용 시 태아에게 장기 신경발달학적 부작용
의 가능성이 있다는 것을 알려야 함.
C
• 제한적 증거에 근거하여, Carbamazepine과 lamotrigine 은 태아에게 신경발달학적 부작
용이 없는 것으로 보임. Levetiracetam과 phenytoin은 증거가 별로 없음. 부모에게 장기
예후는 적은 수의 아동에 근거한 증가라는 것을 알려야 함.
8.
선천성 기형의 최소화
√
•모든 WWE에게 하루에 5mg의 엽
산을 수태 이전부터 최소한 1삼분
기까지 복용하도록 권해야 함.
C
• 임신전 엽산 5mg/d 는 AED관련
인지 저하 위험을 줄이는데 도움이
됨.
B
• 가장 적절한 AED의 효과적인 최소
용량을 사용해야 함.
√
• 수태 전 약제 변경을 통하여,
Sodium valproate와 AED 다약제
복용은 최소화하도록 함.
9.
Antiepileptic
Major Congenital
Malformations
Cognitive Imp
airment
BirthDefects
Valproate Substantial risk Likely
Neural tube, facial clefts, and
possibly hypospadias
Carbamazepine
Likely no substantial
risk
Probably not Posterior cleft palate
Lamotrigine
Possibly no substantial
risk
Probably not Not mentioned
Phenobarbital Not mentioned Possibly
Possible cardiac
malformations
Phenytoin
Possibly no substantial
risk
Possibly Cleft palate
http://www.medscape.com/viewarticle/702006#vp_2
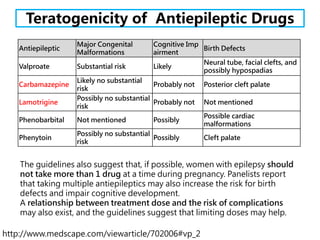
The guidelines also suggest that, if possible, women with epilepsy should
not take more than 1 drug at a time during pregnancy. Panelists report
that taking multiple antiepileptics may also increase the risk for birth
defects and impair cognitive development.
A relationship between treatment dose and the risk of complications
may also exist, and the guidelines suggest that limiting doses may help.
Teratogenicity of Antiepileptic Drugs
10.
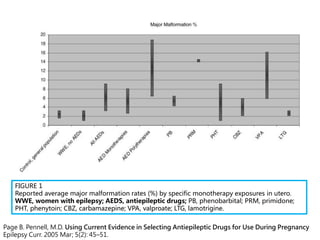
FIGURE 1
Reported averagemajor malformation rates (%) by specific monotherapy exposures in utero.
WWE, women with epilepsy; AEDS, antiepileptic drugs; PB, phenobarbital; PRM, primidone;
PHT, phenytoin; CBZ, carbamazepine; VPA, valproate; LTG, lamotrigine.
Page B. Pennell, M.D. Using Current Evidence in Selecting Antiepileptic Drugs for Use During Pregnancy
Epilepsy Curr. 2005 Mar; 5(2): 45–51.
11.
https://www.epilepsysociety.org.uk/nice-guidelines-anti-epileptic-drugs
PREGNANCY:
The lowest effectivedose of the most appropriate AED should
be used, aiming for monotherapy where possible.
Recent pregnancy databases have suggested that valproate is
significantly more teratogenic than carbamazepine, and the
combination of valproate sodium and lamotrigine is particularly
teratogenic.
Most pregnancies are uneventful in women with epilepsy, and
most babies are delivered healthy with no increased risk of
obstetric complications in women.
Crawford P. Best practice guidelines for the management of women with epilepsy.
Epilepsia. 2005;46 Suppl 9:117-24.
12.
seizure가 임신에 미치는영향
C
• WWE에게 3분의 2는 임신
중 seizure가 심해지지 않는
다는 것을 알려야 함.
D
• 수태 1년이내 seizure를 경
험한 임신부는 집중 관찰을
요함.
Women taking AEDs관리
• 임신 중 routine monitoring of serum
AED levels 는 권고되지 않음 (C)
• 임신부에게 우울, 불안, 신경정신과 증상이
있는지 관심 (D)
• WWE 및 AEDs 복용 임신부에게 산과적 합
병증은 비록 작지만 증가 (B)
15.
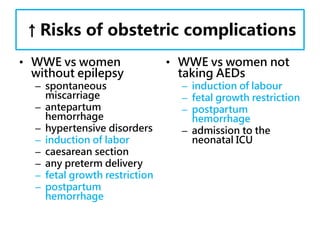
↑Risks of obstetriccomplications
• WWE vs women
without epilepsy
– spontaneous
miscarriage
– antepartum
hemorrhage
– hypertensive disorders
– induction of labor
– caesarean section
– any preterm delivery
– fetal growth restriction
– postpartum
hemorrhage
• WWE vs women not
taking AEDs
– induction of labour
– fetal growth restriction
– postpartum
hemorrhage
– admission to the
neonatal ICU
16.
WWE 관리
• seizure위험 요인 정기 평가 (√ )
– 수면 부족
– 스트레스
– AEDs유지 여부
– seizure 유형과 빈도
• 입원 시 환경에 seizure위험성 고려, 보호자의
지속 관찰(√)
17.
AEDs 노출 태아관리
• Serial growth scans 통하여 small-for-
gestational-age babies 발견 (B)
• routine antepartum fetal surveillance
with cardiotocography 의미 없음 (D)
18.
Vitamin K inpreventing
hemorrhagic disease
• WWE taking enzyme-inducing AEDs 에게
서 태어난 모든 신생아는 출혈 질환 예방 위해
1 mg of vitamin K (IM) 하도록(√)
• 임신부가 경구 vitamin K 복용이 신생아 출혈
질환 예방에 대한 증거는 부족(D)
• WWE에게 vitamin K 권고가 산후 출혈을 예
방한다는 증거도 부족(√)
#14 Pregnant WWE tend to overestimate the risks of teratogenicity associated with intake of
AEDs in pregnancy. Risk perception is likely to have an effect on adherence to AEDs in
pregnancy.52
Women have concerns regarding the effect of epilepsy and its treatment on motherhood.
This includes fear of harming the baby or not being able to fulfil the role of mother to
their expectations.54 Maternal and neonatal death from drowning is a known risk and
mothers should be advised to bathe themselves or their children in shallow water and with
assistance to minimize this risk.6
#19 Enzyme-inducing AEDs (carbamazepine, phenytoin, phenobarbital, primidone, oxcarbazepine,
topiramate and eslicarbazepine) are considered to competitively inhibit the precursors of
clotting factors and affect fetal microsomal enzymes that degrade vitamin K, thereby
increasing the risk of haemorrhagic disease of the newborn. A systematic review to assess
the effect of prenatal vitamin K in preventing haemorrhagic disease of the newborn in WWE
taking enzyme-inducing AEDs did not identify any randomised trials.72 Two observational
studies failed to show a beneficial effect for prenatal vitamin K to prevent haemorrhagic
disease of the newborn,73,74 although it is worth noting that babies in these studies were
also routinely administered 1 mg of vitamin K injection at birth. Despite the lack of objective
evidence, however, it seems reasonable to offer parenteral vitamin K supplementation
routinely to all babies born to mothers on enzyme-inducing AEDs.
#21 Tonic-clonic seizures occur in about 1–2% of WWE in labour and within 24 hours of delivery
in a further 1–2%.77 The EURAP registry reported the occurrence of seizures in 3.5%
(60/1956) of WWE in labour.78
Seizures in labour may lead to maternal hypoxia (due to apnoea during the seizure), and
fetal hypoxia and acidosis secondary to uterine hypertonus.22,79
Prophylactic clobazam is considered in the following circumstances:
recent convulsive seizures, recent history of seizure provocation by stress or sleep
deprivation, or a history of seizures in previous labour. The risks from clobazam, such as
respiratory depression in the newborn, need to be balanced against the benefit due to seizure
prevention.