This document provides an overview of shock in children, including:
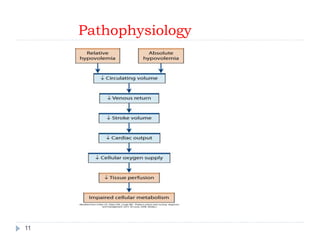
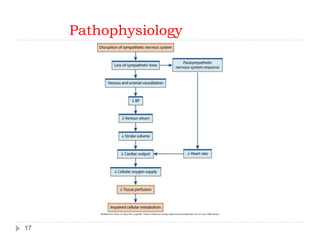
1. It defines shock and describes the pathophysiology involving reduced tissue perfusion and oxygen delivery.
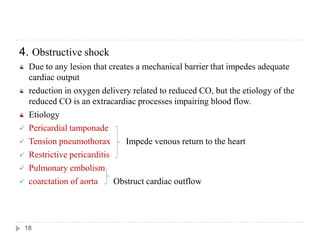
2. It classifies the main types of shock as hypovolemic, cardiogenic, distributive, obstructive, and septic shock and discusses their causes.
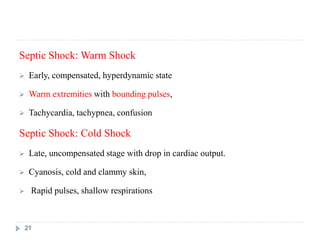
3. It describes the stages of shock from compensated to decompensated to irreversible, and the clinical manifestations including vital signs and mental status changes.
4. It outlines the approach to evaluating a child in shock including history, physical exam focusing on appearance, breathing and circulation, vital signs, mental status, and initial investigations.
5.





































































![PEDIATRICS_SHOCK_MANAGMENT.pptx1114[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pediatricsshockmanagment-230702193650-dab388b8-thumbnail.jpg?width=640&height=640&fit=bounds)



























