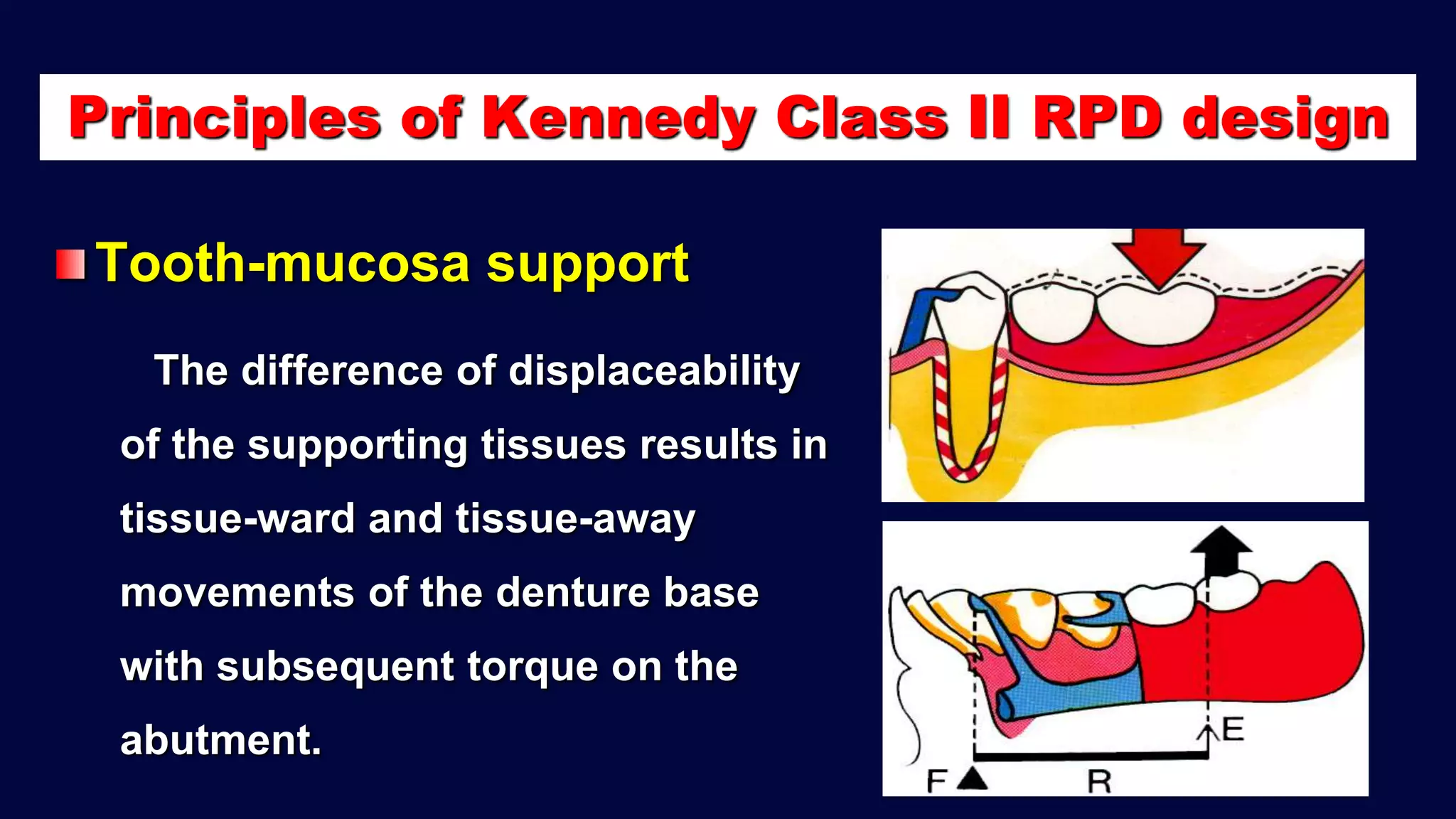
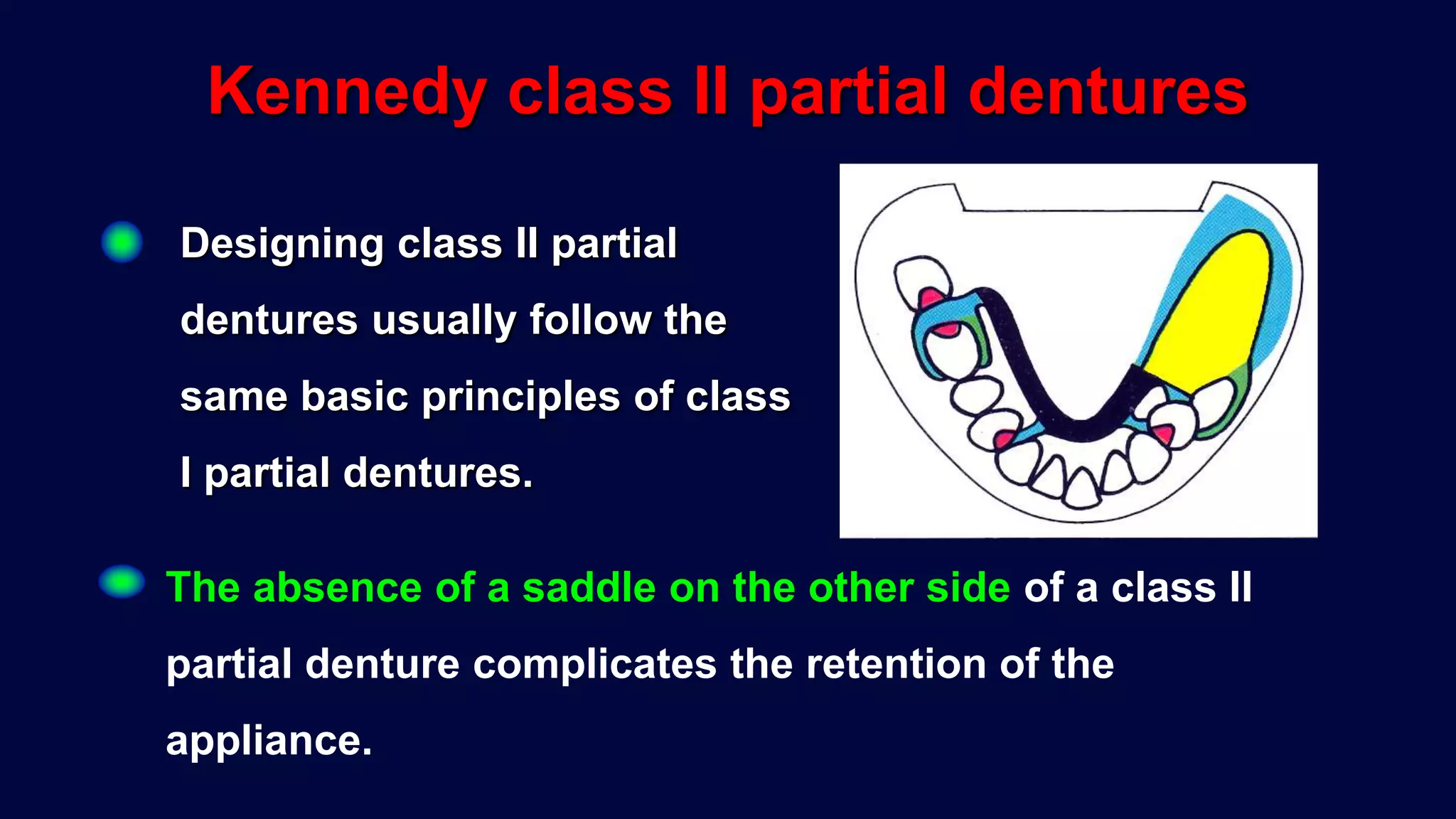
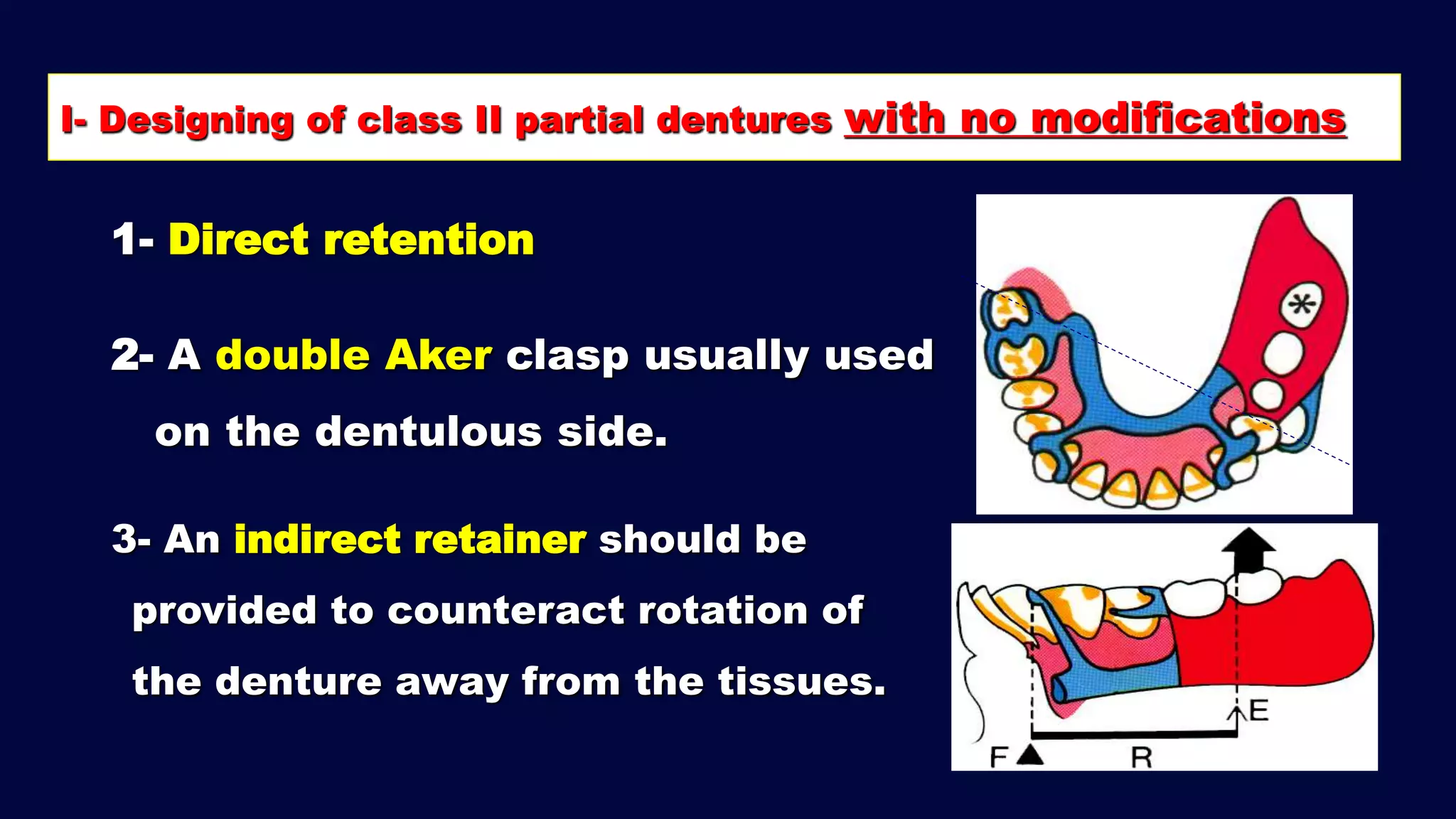
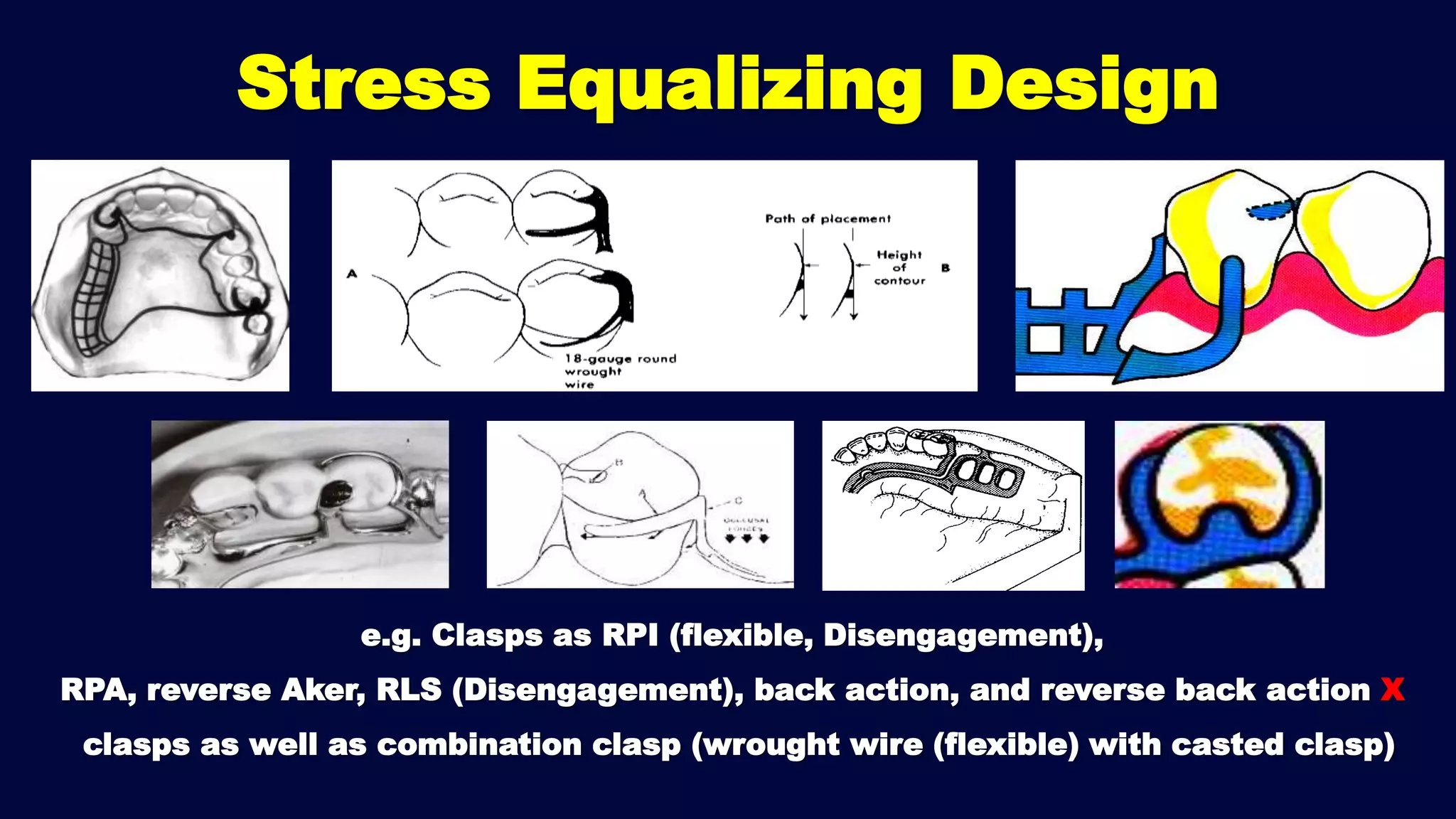
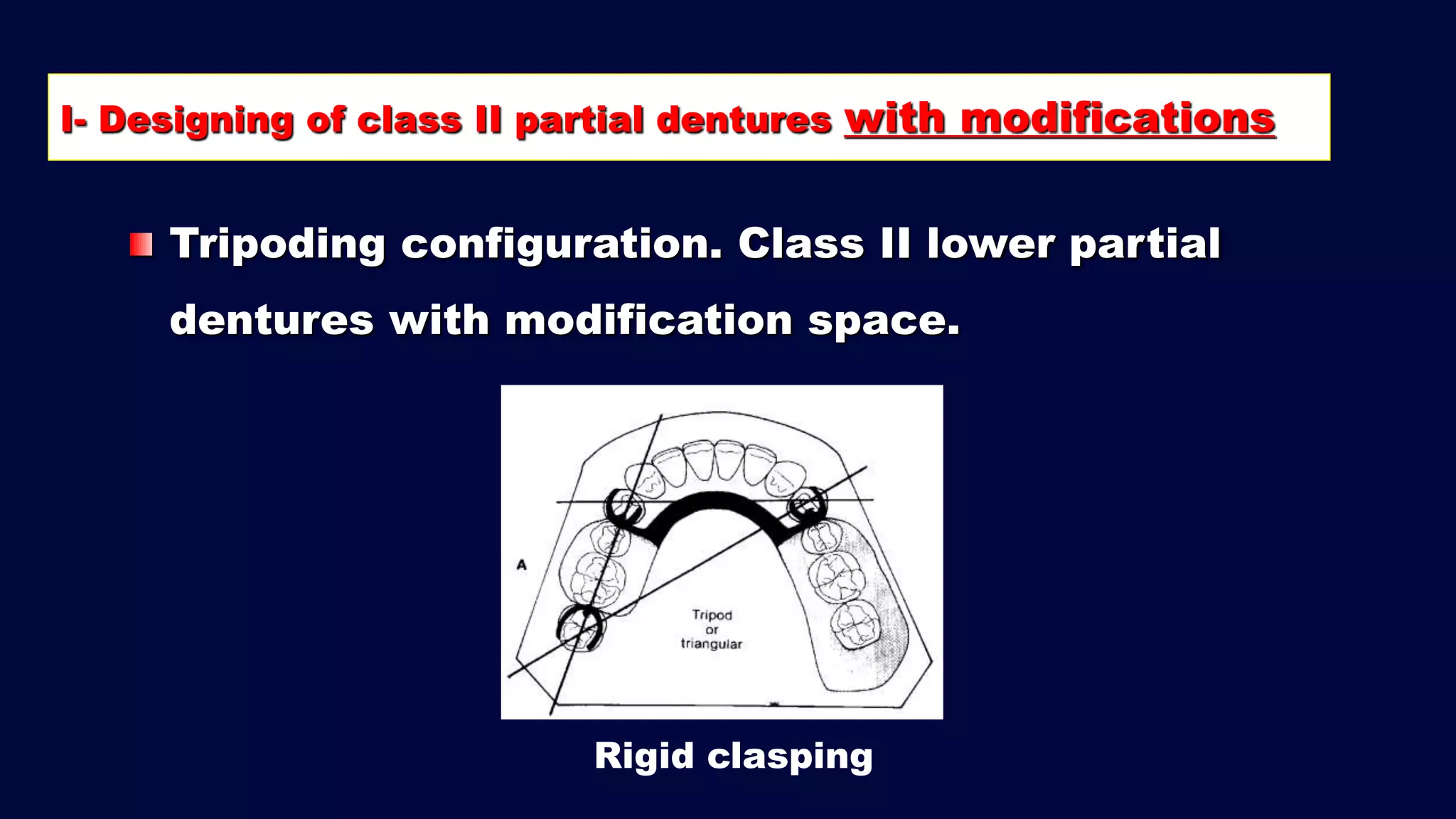
The document discusses principles of removable partial denture design. It covers factors that influence design like forces in the mouth and conditions of the ridges and abutment teeth. It also discusses biomechanical principles like support, retention, bracing and stabilization. Specific principles for Kennedy class designs are outlined, including the importance of tissue coverage, indirect retention, and stress equalizing components to minimize strain. Modifications for longer edentulous spans are also noted.