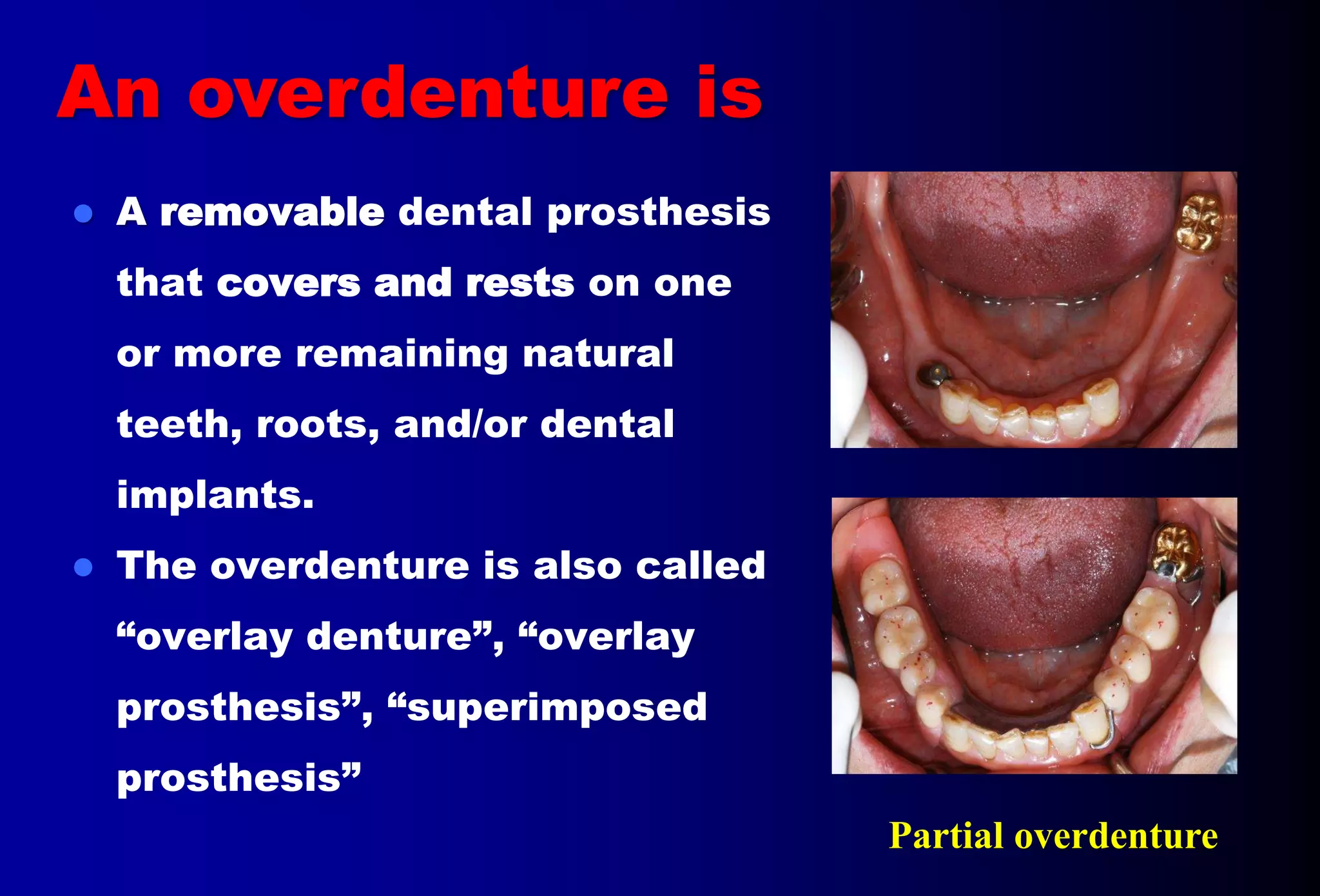
An overdenture is a removable partial or complete denture that covers and rests on one or more remaining natural teeth, dental implants, or dental abutments. This document discusses definitions, types, indications, contraindications, advantages, and disadvantages of overdentures. It also covers factors to consider when selecting teeth for overdentures such as periodontal health, endodontic needs, tooth position and number. The document outlines the treatment planning process and protocols for laboratory and clinical procedures for overdentures.