



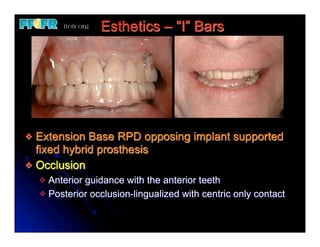





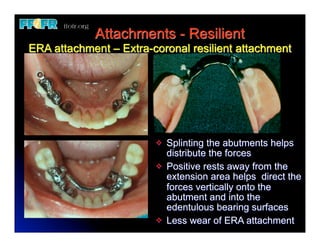











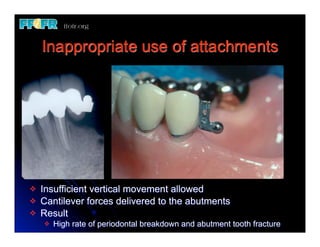

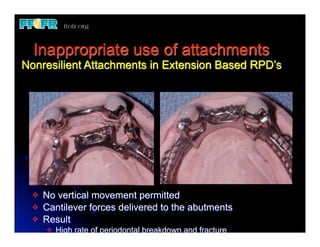



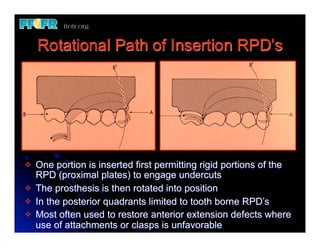

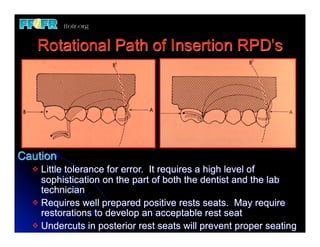
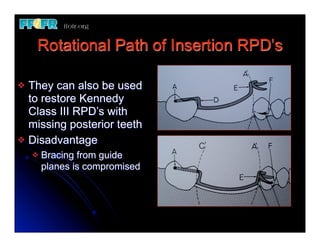


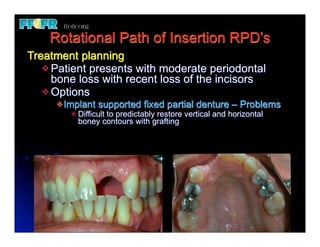
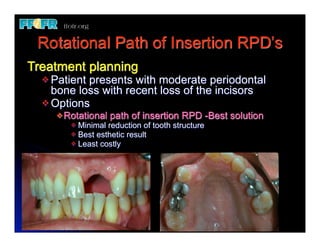
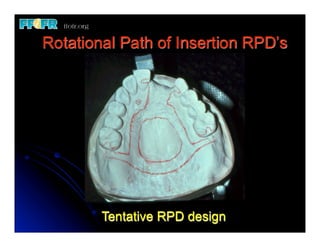
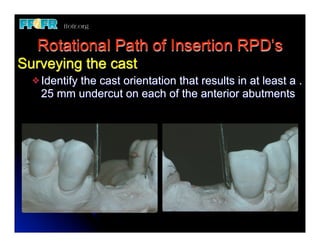

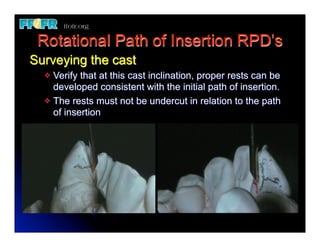





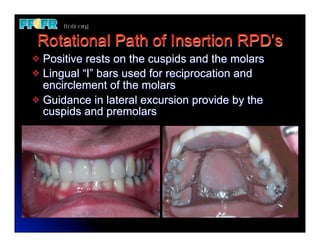
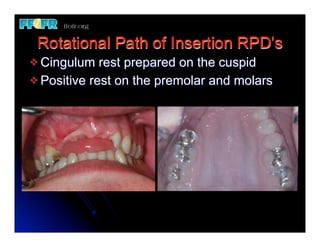



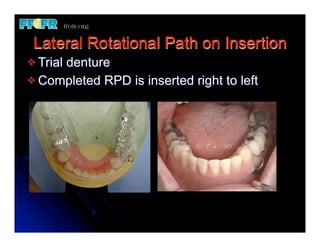


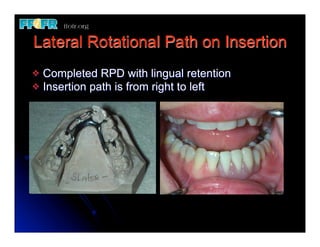

This presentation discusses different prosthodontic treatment options including the use of attachments, rotational path RPDs, and lateral rotational path RPDs. It provides examples of how attachments like the ERA can be used to improve esthetics and distribute forces. Rotational path and lateral rotational path RPDs are described as alternatives to clasped RPDs that can eliminate visible clasps. Factors like positive rests and undercuts are emphasized for successful use of these techniques. Inappropriate uses of attachments that deliver cantilever forces are also highlighted.



































































