Download as PPSX, PPTX

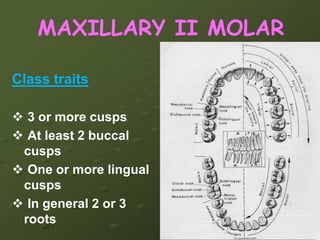
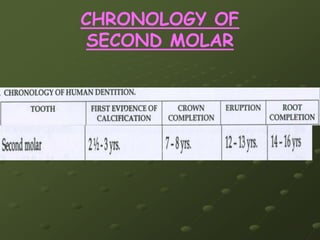
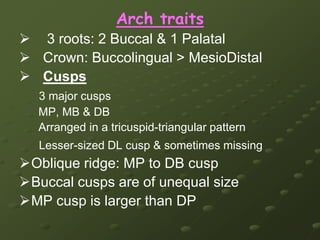
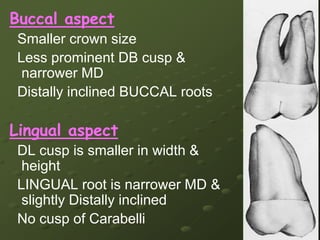
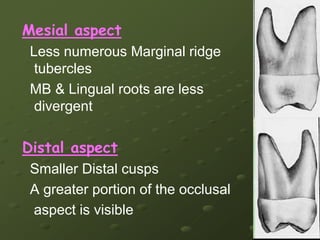
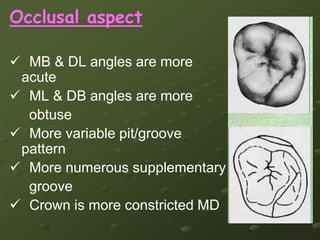
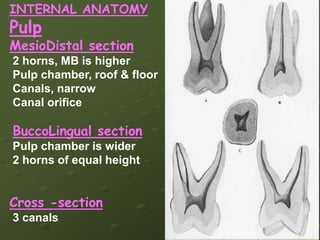
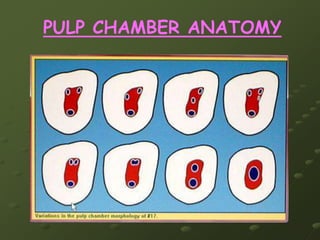
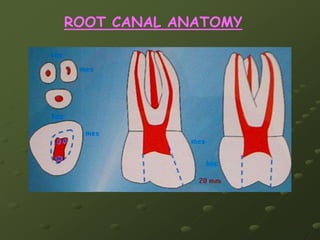
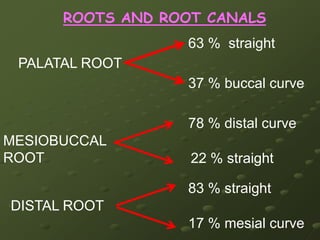
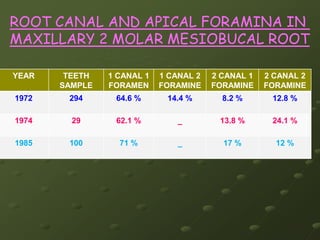
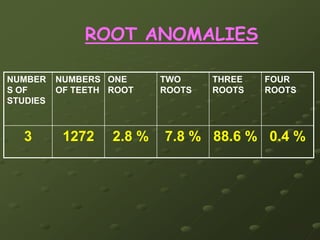
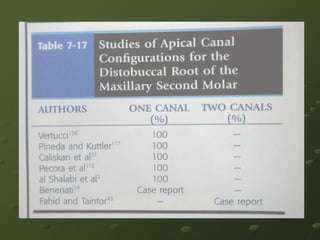
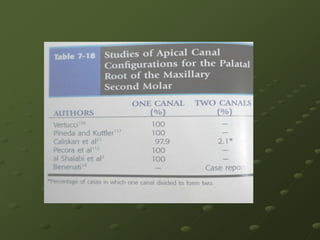

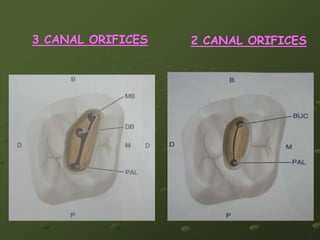
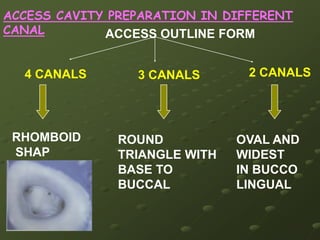

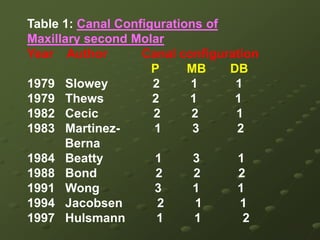

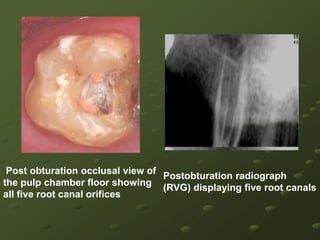



This document discusses the anatomy and endodontic treatment of maxillary second molars. It begins with the external and internal anatomy, including descriptions of the crown, roots, root canals, pulp chamber, and anomalies. It then covers topics like eruption timing, root curvatures, access cavity preparation, working length determination, and management of complex anatomies like calcified canals. Case reports are also presented, such as a tooth with two canals in the palatal root. In summary, the document provides a comprehensive overview of maxillary second molar anatomy and its relevance to endodontic treatment.



































































