BRIEF HISTORY OFSPINAL ANAESTHESIA
CSF DISCOVERED –BY Domenico catugno 1764
CSF CIRCULATION-by F. Magendie 1825
FIRST SPINAL ANAESTHESIA - by J leonard corning 1885
FIRST PLANED SPINAL ANAESTHESIA ON HUMANS -by august bier in
1891 using cocaine
USING BUPIVACAINE BY EMBLEM IN 1966.
3.
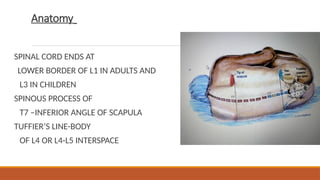
Anatomy
SPINAL CORD ENDSAT
LOWER BORDER OF L1 IN ADULTS AND
L3 IN CHILDREN
SPINOUS PROCESS OF
T7 –INFERIOR ANGLE OF SCAPULA
TUFFIER’S LINE-BODY
OF L4 OR L4-L5 INTERSPACE
4.
Vertebral column
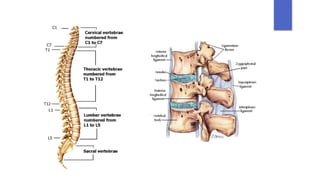
▶ Consistsof 33 vertebrae: 7 cervical, 12 thoracic, 5 lumbar, 5 fused sacral
vertebrae and a rudimentary coccyx (4 segments)
▶ Vertebra consists of a body and a hollow ring defined anteriorly by the
vertebral body, laterally by pedicles and transverse process and posteriorly
by lamina and spinal processes
▶ The hollow rings form the spinal canal which contains the spinal cord and
its coverings
▶ There are four synovial joints (facet joints adjacent to the transverse
processes). Two articulate with the vertebra above and two with the
vertebra below
5.
▶ Pedicles arenotched superiorly and inferiorly.
These notches form the intervertebral foramina
thorugh which the spinal nerves exit
▶ Laminae of the S5 and all or part of S4 normally
do not fuse, leaving a caudal opening to the
spinal canal, the sacral hiatus
▶ Spinal column forms a double C, being convex
anteriorly in the cervical and lumbar regions
▶ Vertebral bodies and intervertebral discs are
connected and supported by ligaments
▶ Ventrally: anterior and posterior longitudinal
ligament
▶ Dorsally: ligamentum flavum, interspinous
ligament, supraspinous ligament
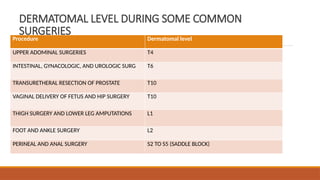
DERMATOMAL LEVEL DURINGSOME COMMON
SURGERIES
Procedure Dermatomal level
UPPER ADOMINAL SURGERIES T4
INTESTINAL, GYNACOLOGIC, AND UROLOGIC SURG T6
TRANSURETHERAL RESECTION OF PROSTATE T10
VAGINAL DELIVERY OF FETUS AND HIP SURGERY T10
THIGH SURGERY AND LOWER LEG AMPUTATIONS L1
FOOT AND ANKLE SURGERY L2
PERINEAL AND ANAL SURGERY S2 TO S5 (SADDLE BLOCK)
9.
CEREBROSPINAL FLUID
CSF isa clear watery fluid contained within the cerebral ventricles and the
subarachnoid space
Total volume of CSF about 100-160 ml
It is ultra filtrate formed by active process from choroid plexus of lateral ventricles
The epidymal cells of pia covering the blood vessels play secretary role
500-600ml of CSF formed per day
About 20-25 ml is present in ventricles ,90ml in reservoirs in brain,25-30 ml occupy
the sub arachnoid space
It is produced at a rate of 0.4ml/min ,it is around 25ml/hr
.
10.
Cerebrospinal fluid
The specificgravity of CSF is 1.003-
1.009
It’s PH is 7.4 – 7.6
Na - 140- 150 meq/L
Chloride - 120-130 meq/L
Bicarbonate - 25 -30 meq/L
Proteins - 15-45 mg/dl
Glucose - 50-80 mg/dl
Baricity - Density of a solution in
relation to density of CSF
Hypobaric solutions :raise against
gravity
Isobaric solutions : tends to
remain in same sight where they
are injected
Hyperbaric solutions : tend to
follow gravity
11.
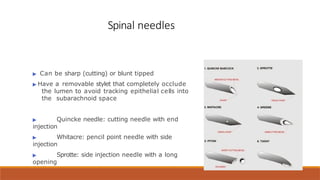
Spinal needles
▶ Canbe sharp (cutting) or blunt tipped
▶ Have a removable stylet that completely occlude
the lumen to avoid tracking epithelial cells into
the subarachnoid space
▶ Quincke needle: cutting needle with end
injection
▶ Whitacre: pencil point needle with side
injection
▶ Sprotte: side injection needle with a long
opening
12.
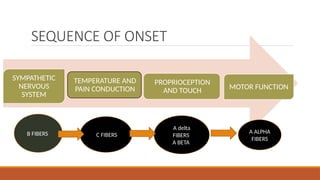
Mechanism of actionof nerve blockade
Generally ,autonomic and sensory fibers are blocked before motor fibers leading
to several important consequences
Local anesthetics interacts with the receptor situated within the voltage sensitive
sodium channel and raises the threshold of channel opening
Decreases the entry of sodium ions during upstroke of action potential
Local depolarization fails to reach the threshold potential and conduction block
occurs
Onset time of blockade is related to the pKa of the LA
Lower pKa – fast acting
13.
PROCEDURE PREPARATION
REMOVE YOURJEWELLERY/WATCHES
WASH YOUR HANDS
IV ACCESS/FLUIDS BOLUS IF NEEDED
EMERGENCY DRUGS /EQUIPMENT
POSITION
SEDATION IF NEEDED
MONITORING NIBP/SPO2/ECG
VERBAL CONTACT WITH PATIENT
14.
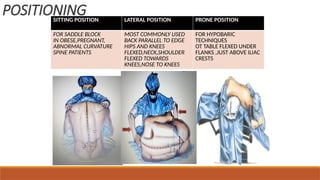
POSITIONING
SITTING POSITION LATERALPOSITION PRONE POSITION
FOR SADDLE BLOCK
IN OBESE,PREGNANT,
ABNORMAL CURVATURE
SPINE PATIENTS
MOST COMMONLY USED
BACK PARALLEL TO EDGE
HIPS AND KNEES
FLEXED,NECK,SHOULDER
FLEXED TOWARDS
KNEES,NOSE TO KNEES
FOR HYPOBARIC
TECHNIQUES
OT TABLE FLEXED UNDER
FLANKS ,JUST ABOVE ILIAC
CRESTS
Factors affecting blockheight
Technique of injection
-Site of injection
-Direction of injection
-Use of barbotage
-Rate of injection
17.
Technique
Using median orparamedian approach needle is advanced until 2 popups are felt
-penetration of ligamentum flavum
-penetration of dura arachnoid membrane
Inject at rate of 0.2ml/sec ,aspirate small amount of spinal fluid then remove
spinal needle and introducer simultaneously
18.
Technique
Paramedian approach
1 -1.5cm lateral to midline
Spinal needle is inserted at an angle of 25 degrees with the midline and without
deviation from cephalad or caudad
Needle lies lateral to supraspinous and interspinous ligaments bypassing them and
penetrate ligamentum flavum and duramater in midline
It pierces skin ,subcutaneous tissue ,lumbar aponurosis ,ligamentum flavum ,dura and
arachnoid mater
Useful in arthritis ,deformed spine ,kyphoscoliosis,etc.
19.
• A 12cm spinal needle is inserted 1 cm
medially and 1 cm above the lowest
prominence of posterior superior iliac
spine
• Needle is directed upward medially and
forward at an angle of 50 degrees
• Uses : spinal fusion ,arthritic spine,
opisthotonos , skin infection in lumbar
region
Taylor technique
20.
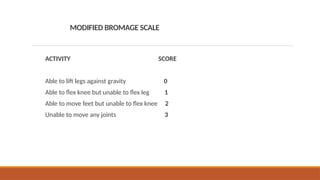
MODIFIED BROMAGE SCALE
ACTIVITYSCORE
Able to lift legs against gravity 0
Able to flex knee but unable to flex leg 1
Able to move feet but unable to flex knee 2
Unable to move any joints 3
20
▶ There isa decrease in blood pressure
▶ Vasomotor tone due to sympathetic fibres arising from T5-
L1 are blocked leading to vasodilatation and pooling of
blood in the viscera and lower extremities
▶ Effects of arterial vasodilatation may be minimized by
compensatory block above the level of the block
▶ High sympathetic block prevent compensatory
vasoconstriction, and can block sympathetic acceleratory
fibres (T1-4). Profound hypotension may develop because
of arterial dilatation, venous pooling and bradycardia
Cardiovascular manifestations
23.
Pulmonary effects
. Thereis only a small decrease in vital capacity due to loss of abdominal
muscles contribution to forced expiration
Patients with COPD may rely upon accessory muscles of respiration to
actively inspire or exhale. High levels of neuraxial block will impair these
muscles
Effective coughing and clearing of secretions can be impaired
Tidal volume remains unchanged
24.
Gastrointestinal effects
▶ Neuraxialblock induced sympathectomy allows vagal tone
dominance and results in small contracted gut with active
peristalsis
▶ This can improve operative conditions during laproscopy
when used as an adjunct to general anaesthesia
▶ Postoperative epidural analgesia hastens return of
gastrointestinal function after abdominal procedures
25.
Renal function
▶ Renalblood flow is maintained by autoregulation
and there is little effect of neuraxial anaesthesia on
renal function
▶ Loss of autonomic bladder control results in urinary
retention until the block wears off
26.
Indications
surgeries of lowerlimb, perineum ,pelvis, abdomen
Ideal for
1. Renal failure- onset is rapid ,spread is greater by 2-3 segments ,duration is shorter
2. Cardiac disease
3. Liver disease
4. Obstetric anaesthesia
5. Immunosuppresed patients –does not impair cell mediated immunity
6. Elderly patients
7. Dm patients
27.
contraindications
RELATIVE ABSOLUTE
UNCOPERATIVE PATIENT
PRE-EXISTINGNEUROLOGICAL
DEFICITS
DEMYLINATING LESIONS
SEVERE SPINAL DEFORMITY
INFECTION AT SITE REMOTE
FROM INSERTION
PATIENTS REFUSAL
COAGULOPATHY
INFECTION AT LOCAL SITE
SEVERE HYPOVOLEMIA
INCREASED ICT
ALLERGY TO DRUGS
SHOCk
SEVERE AS OR MS
Hypotension
▶ Prevention andtreatment of Hypotension
▶ Volume loading with 10-20 ml/kg of intravenous fluid
▶ Left uterine displacement in the third trimester of pregnancy
▶ Autotransfusion by placing the patient in a head low position
▶ Vasopressors such as phenylephrine, ephedrine
32.
HIGH NEURAL BLOCKADE,HIGH SPINAL AND TOTAL
SPINAL ANAESTHESIA
Administration of an excessive dose , failure to reduce doses in selected
pts (elderly ,pregnant, obese , very short ) or unusual sensitivity or spread
of LA maybe responsible
SA ascending into cervical level causes severe hypotension , bradycardia
and respiratory insufficiency and even aponea
33.
• TREATMENT –vasopressors (to increase BP ) ,atropine ( to treat
bradycardia ), fluids , oxygen ,assisted ventilation ( to overcome
respiratory insufficiency ) and even intubation and mechanical
ventilation may be needed
34.
Total spinal anaesthesia
Intravenousfluids over shorter timescale. Rapid administration of
crystalloid ,1000 ml ,then colloid ,500 ml . Repeat as necessary to maintain
systolic pressure > 100 mm Hg
Respiratory support (100% oxygen via face mask progressing to assisted manual
ventilation )
Tracheal intubation if unconsciousness occurs
Atropine increment of 0.3 mg ,used to treat bradycardia
35.
• Ephedrine ,10 mg increment to total of 30 mg , to restore
systolic pressure > 100 mm Hg
• Intravenous infusion of epinephrine maybe necessary to
maintain the level of blood pressure until the block to wear
off
• Slight head down tilt ( 10 – 20 degree ) and slight tilting
maybe used to maximize venous return
• maintain supportive measures until level of spinal block
regresses
36.
Post dural punctureheadache (PDPH)
▶ Due to loss of CSF. Low CSF pressure causes traction on nerve roots
and intracranial structures
▶ Typically PDPH is bilateral, frontal, retroorbital or occipital. It may
be throbbing of constant and associated with photophobia,
nausea
▶ Headache is characteristically worse when head is elevated and
becomes milder or relieved when patient is supine
▶ Incidence decreases with small diameter, noncutting, pencil point
needles
37.
▶ Treatment ofPDPH
▶ Alleviation of symptoms
▶ Bed rest: keeping the patient supine will reduce the
hydrostatic pressure driving the CSF out of the dural hole
▶ Fluids and caffeine:
▶ Analgesics: Paracetamol, tramadol
▶ Attempts to seal the hole
▶ Epidural blood patch: 15-20 ml of autologous blood is
injected into the epidural space at or one interspace below.
Further leak of CSF is stopped by mass effect or coagulation.
▶ It may take 1-6 weeks for the symptoms to resolve
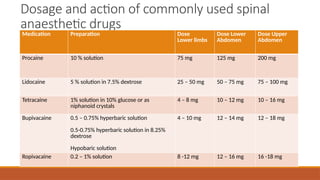
Dosage of drugused
Hyperbaric Bupivacaine –
According to weight
0- 5 kg – 0.5 ml/kg
5-15 kg – 0.4ml/kg
> 15kgs – 0.3ml/kg
According to height ( can be used in
pregnant females )- 0.06 ml/cm of
height
Paediatric drug dosing
Paediatric drug dosage can be
calculated by using
Young’s formula –
Child dose = age/( age + 12 )
multiplied by average adult
dose
40.
Spinal anaesthetic agents
▶Only preservative free local anaesthetic solutions are used
▶ Local anaesthetic properties
▶ Potency is related to lipid solubility
▶ Duration of action is affected by protein binding
▶ Onset of action is related to amount of local anaesthetic
available in the base form
▶ Hyperbaric bupivacaine and tetracaine are commonly used
agents.
have relatively slow onset (5-10 min) and prolonged duration (90-120
min)
▶ Lidocaine and procaine have a rapid onset (3-5 min) and short
duration of action (60-90 min)
▶ Lidocaine is associated with transient neurological symptoms and
cauda equine
41.
Additives to localanaesthesia
▶ Addition of vasoconstrictors and opioids enhance the quality
and prolong the duration of spinal anaesthesia
▶ Following drugs can be used as additives
▶ Epinephrine (0.1-0.5mg)
▶ Opioids (Fentanyl, sufentanil, meperidine, morphine)
▶ Alpha 2 agonists (clonidine)
▶ Acetylchoinesterase inhibitors (neostigmine)
42.
Spinal anaesthesia inpregnancy
Decreased dose requirement due to
Mechanical factors : compression of IVC causes
shunting of blood to venous plexus in vertebral
canal
Decreased vertebral canal space and CSF volume
Hormonal factors : higher progesterone levels
43.
ADVANTAGES OF SPINALANAESTHESIA
(SPA)
1. The costs associated with SPA are minimal
2. Patient satisfaction : majority of patients are very happy with this technique.
3. Respiratory diseases : few adverse effects on respiratory system.
4. Patent airway: reduced risk of airway obstruction or aspiration of gastric
contents.
5. Diabetic patients : little risk of unrecognised hypoglycemia in an awake patient.
44.
• Muscle relaxation: excellent muscle relation for lower
abdominal and lower limb surgery.
• Bleeding :less blood loss.
• Splanchnic blood flow : reduces incidence of
anastomotic dehiscence.
• Visceral tone : normal gut function rapidly returns
following surgery.
• Coagulation : post-operative deep vein thromboses and
pulmonary emboli are less common