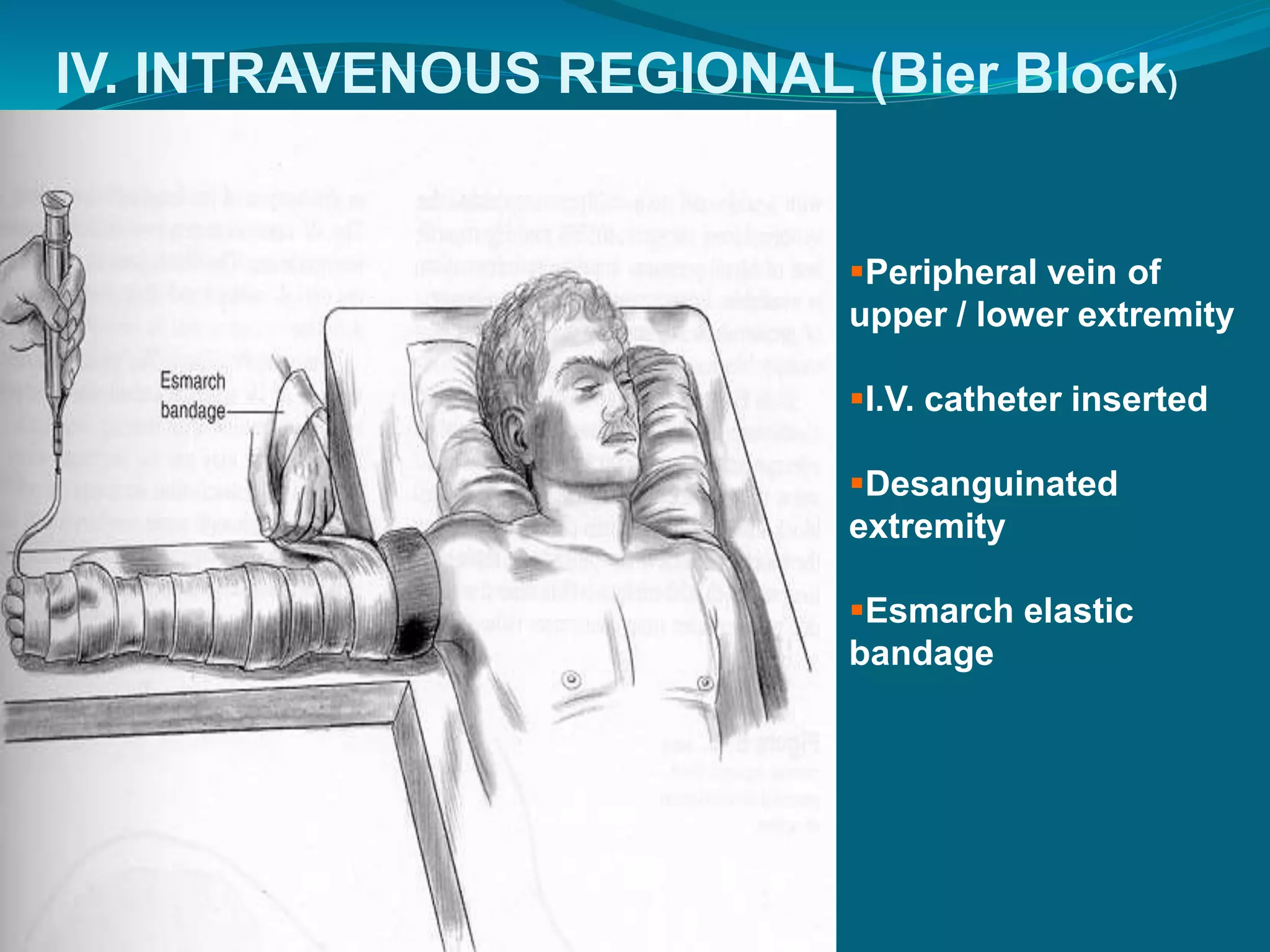
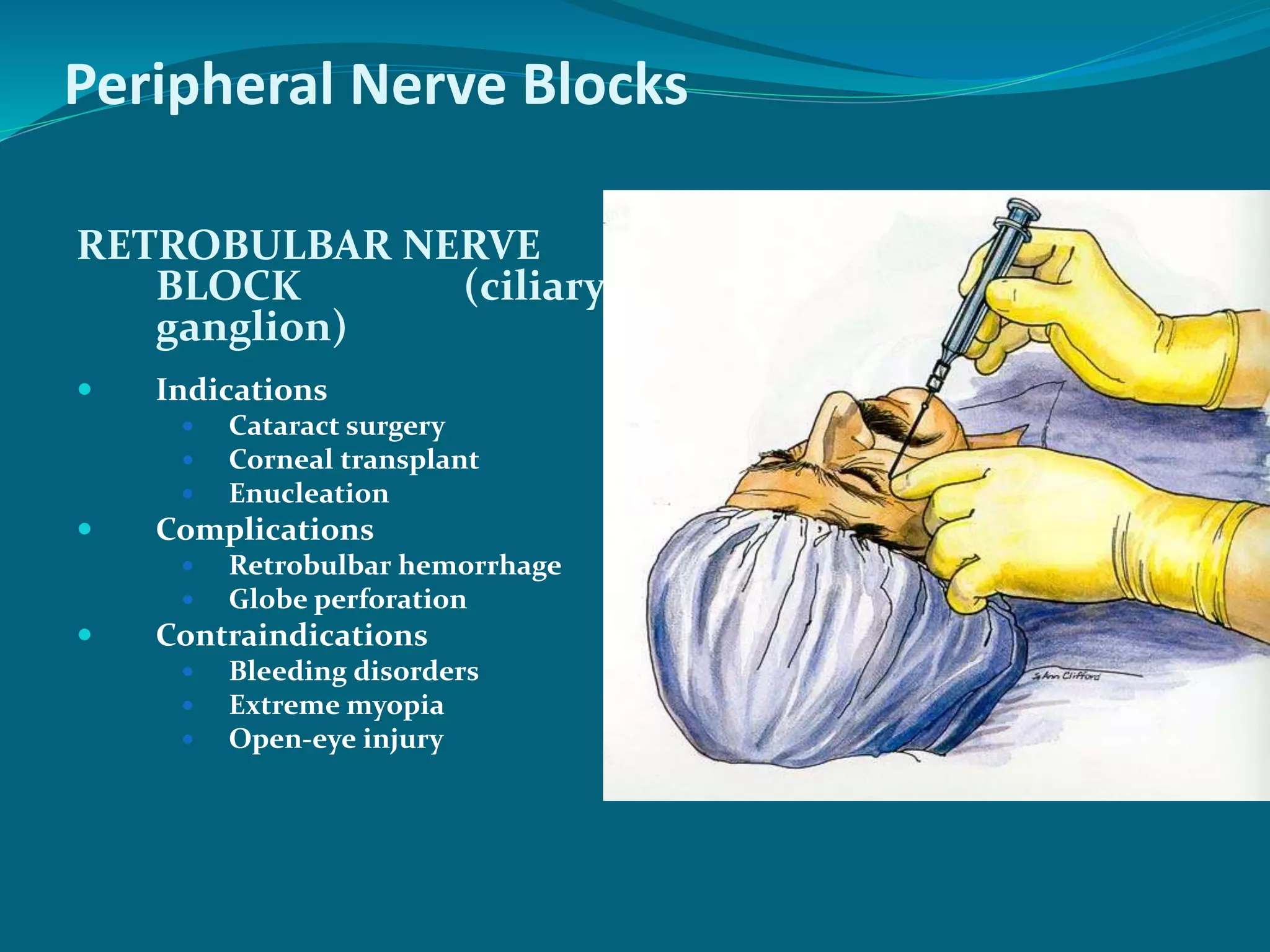
This document discusses regional anesthesia techniques. It begins by explaining nerve physiology and conduction. It then classifies regional anesthesia based on the site of local anesthetic application, including topical, infiltration, field block, and intravenous regional anesthesia. The document describes various peripheral nerve blocks such as interscalene brachial plexus block, ankle block, and dorsal penile block. It also discusses central (neuroaxial) blocks like spinal anesthesia, epidural anesthesia, and caudal anesthesia, explaining their indications, techniques, effects, advantages, and disadvantages.