Presentation for a lecture on_Anesthesia_part_3.pptx
1.
Anesthesiology
Local anesthetics ®ional
anesthesia
Anesthesiology, Reanimatology & Intensive care Faculty
with Ambulance/Paramed course. TSMU of RF Health ministry
Anesthesiology
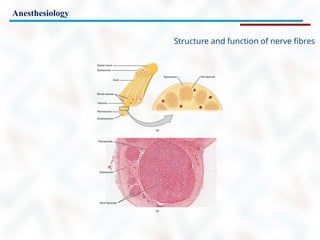
Structure and functionof nerve fibres
Diagram showing transverse section of (a) myelinated nerve fibres an
(b) unmyelinated nerve fibres.
A – axon or dendrite; m – myelin sheath; sn – nucleus of Schwann cell.
7.
Anesthesiology
Structure and functionof nerve fibres
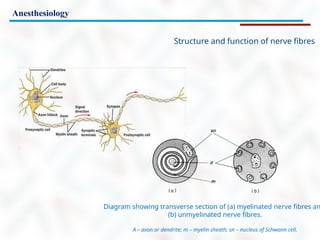
Myelinated axon.
A – The diagram shows a cross section of an axon and its coverings formed by a Schwann cell:
the myelin sheath and neurilemma. B – Transmission electron micrograph showing how the
densely wrapped layers of the Schwann cell’s plasma membrane form the fatty myelin sheath
8.
Anesthesiology
Structure and functionof nerve fibres
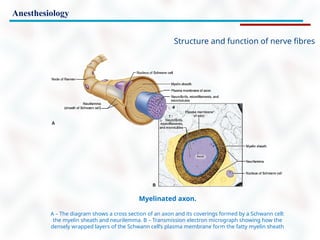
Compound Aα, Aδ, and C fiber action potentials recorded after supramaximal stimulation of a rat
sciatic nerve.
Note the differing time scale of the recordings. In peripheral nerves, Aδ and C fibers have much slower
conduction velocities, and their compound action potentials are longer and of less amplitude when compared with
those from Aα fibers.
9.
Anesthesiology
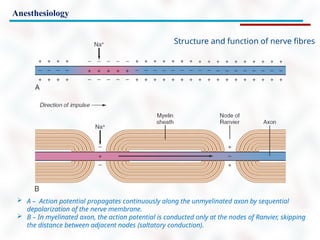
A –Action potential propagates continuously along the unmyelinated axon by sequential
depolarization of the nerve membrane.
B – In myelinated axon, the action potential is conducted only at the nodes of Ranvier, skipping
the distance between adjacent nodes (saltatory conduction).
Structure and function of nerve fibres
Anesthesiology
Ionic (sodium ion[Na+]) currents measured by voltage-clamp technique by depolarization
applied infrequently (“tonic” test). After equilibration with 0.2 mM lidocaine, the currents measured tonically
are reduced significantly compared with control currents. Application of repeate depolarizations results in a
dynamic reduction of currents after each depolarization (use-dependent inhibition).
Modified from Butterworth JF, Strichartz GR. Molecular mechanisms of local anesthesia: a review
Anesthesiology 1990;72:711–734.
Structure and function of nerve fibres
Anesthesiology
Decremental decay
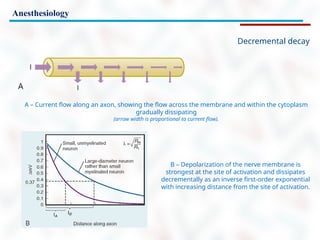
A –Current flow along an axon, showing the flow across the membrane and within the cytoplasm
gradually dissipating
(arrow width is proportional to current flow).
B – Depolarization of the nerve membrane is
strongest at the site of activation and dissipates
decrementally as an inverse first-order exponential
with increasing distance from the site of activation.
Anesthesiology
Regional Anesthetic techniques
Infiltration Anesthesia
Central neuraxial anesthesia
Spinal anesthesia
Epidural Anesthesia
Combined Epidural and Spinal
Anesthesia
IV Regional Block
Peripheral Nerve Blocks
28.
Anesthesiology
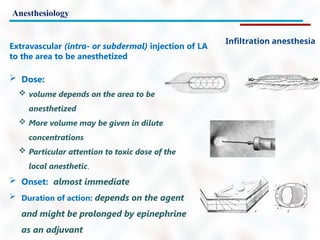
Infiltration anesthesia
Dose:
volume depends on the area to be
anesthetized
More volume may be given in dilute
concentrations
Particular attention to toxic dose of the
local anesthetic.
Onset: almost immediate
Duration of action: depends on the agent
and might be prolonged by epinephrine
as an adjuvant
Extravascular (intra- or subdermal) injection of LA
to the area to be anesthetized
29.
Anesthesiology
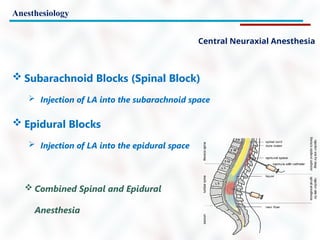
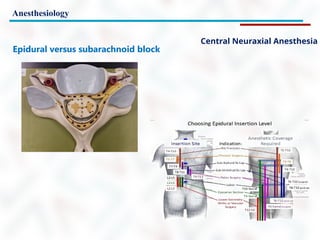
Central Neuraxial Anesthesia
Subarachnoid Blocks (Spinal Block)
Injection of LA into the subarachnoid space
Epidural Blocks
Injection of LA into the epidural space
Combined Spinal and Epidural
Anesthesia
30.
Anesthesiology
Indications
Might beused alone or in conjunction with GA for most
procedures below the neck
Most useful for:
lower abdominal
inguinal
urogenital
rectal
lower extremity surgery
*Lumbar spinal surgery may also be performed under spinal anesthesia
Upper abdominal procedures
difficult to achieve a sensory level adequate for patient comfort yet
avoid the complications of a high block
Spinal anesthesia for neonatal surgery
31.
Anesthesiology
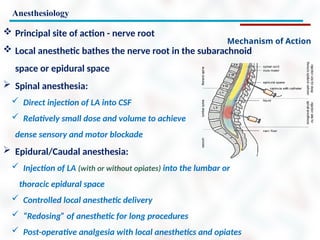
Mechanism of Action
Principal site of action - nerve root
Local anesthetic bathes the nerve root in the subarachnoid
space or epidural space
Spinal anesthesia:
Direct injection of LA into CSF
Relatively small dose and volume to achieve
dense sensory and motor blockade
Epidural/Caudal anesthesia:
Injection of LA (with or without opiates) into the lumbar or
thoracic epidural space
Controlled local anesthetic delivery
“Redosing” of anesthetic for long procedures
Post-operative analgesia with local anesthetics and opiates
32.
Anesthesiology
Spinal Anesthesia
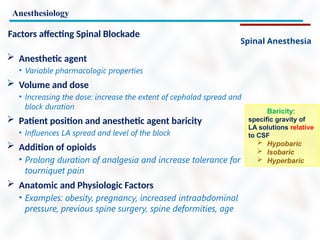
Factors affectingSpinal Blockade
Anesthetic agent
• Variable pharmacologic properties
Volume and dose
• Increasing the dose: increase the extent of cephalad spread and
block duration
Patient position and anesthetic agent baricity
• Influences LA spread and level of the block
Addition of opioids
• Prolong duration of analgesia and increase tolerance for
tourniquet pain
Anatomic and Physiologic Factors
• Examples: obesity, pregnancy, increased intraabdominal
pressure, previous spine surgery, spine deformities, age
Baricity:
specific gravity of
LA solutions relative
to CSF
Hypobaric
Isobaric
Hyperbaric
33.
Anesthesiology
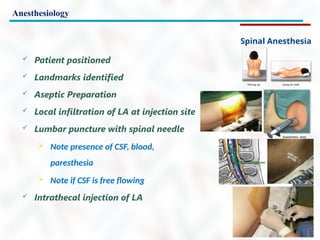
Spinal Anesthesia
Patientpositioned
Landmarks identified
Aseptic Preparation
Local infiltration of LA at injection site
Lumbar puncture with spinal needle
Note presence of CSF, blood,
paresthesia
Note if CSF is free flowing
Intrathecal injection of LA
34.
Anesthesiology
Central Neuraxial Anesthesia
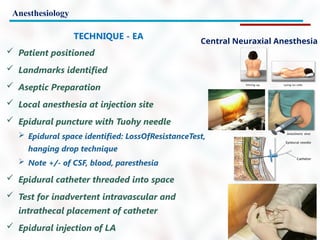
TECHNIQUE- EA
Patient positioned
Landmarks identified
Aseptic Preparation
Local anesthesia at injection site
Epidural puncture with Tuohy needle
Epidural space identified: LossOfResistanceTest,
hanging drop technique
Note +/- of CSF, blood, paresthesia
Epidural catheter threaded into space
Test for inadvertent intravascular and
intrathecal placement of catheter
Epidural injection of LA
Anesthesiology
Central Neuraxial Anesthesia
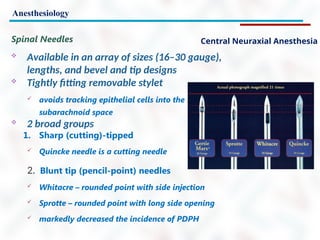
SpinalNeedles
Available in an array of sizes (16–30 gauge),
lengths, and bevel and tip designs
Tightly fitting removable stylet
avoids tracking epithelial cells into the
subarachnoid space
2 broad groups
1. Sharp (cutting)-tipped
Quincke needle is a cutting needle
2. Blunt tip (pencil-point) needles
Whitacre – rounded point with side injection
Sprotte – rounded point with long side opening
markedly decreased the incidence of PDPH
Anesthesiology
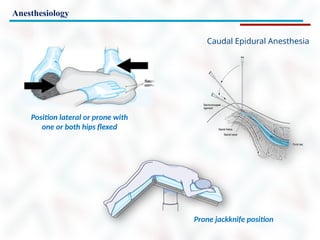
Caudal Epidural Anesthesia
One of the most commonly used regional
techniques in pediatric patients
Used in anorectal surgery in adults
2nd
stage of labor
In children - typically combined with GENA
for intraop supplementation and postop analgesia
Performed after induction
Commonly used for procedures below the diaphragm
urogenital, rectal, inguinal, and lower extremity
Within the sacral canal, the dural sac extends to…what level?
S2 in adults
S3 in infants
Makes inadvertent intrathecal injection much more common
in infants
Anesthesiology
Intravenous Regional Anesthesia
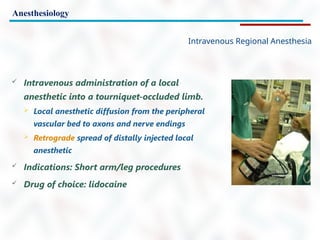
Intravenous administration of a local
anesthetic into a tourniquet-occluded limb.
Local anesthetic diffusion from the peripheral
vascular bed to axons and nerve endings
Retrograde spread of distally injected local
anesthetic
Indications: Short arm/leg procedures
Drug of choice: lidocaine
43.
Anesthesiology
Intravenous Regional Anesthesia
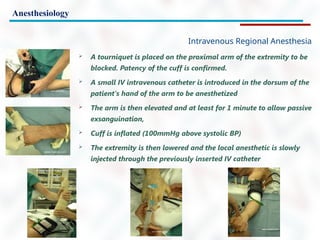
A tourniquet is placed on the proximal arm of the extremity to be
blocked. Patency of the cuff is confirmed.
A small IV intravenous catheter is introduced in the dorsum of the
patient's hand of the arm to be anesthetized
The arm is then elevated and at least for 1 minute to allow passive
exsanguination,
Cuff is inflated (100mmHg above systolic BP)
The extremity is then lowered and the local anesthetic is slowly
injected through the previously inserted IV catheter
44.
Anesthesiology
Intravenous Regional Anesthesia
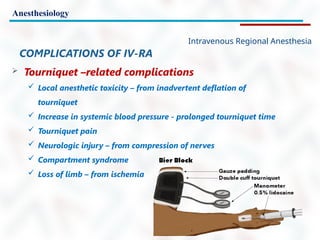
COMPLICATIONSOF IV-RA
Tourniquet –related complications
Local anesthetic toxicity – from inadvertent deflation of
tourniquet
Increase in systemic blood pressure - prolonged tourniquet time
Tourniquet pain
Neurologic injury – from compression of nerves
Compartment syndrome
Loss of limb – from ischemia
Reversal Agents/Anticholinergics
Reversal Agents:all are acetylcholinesterase inhibitors, thereby allowing
more acetylcholine to be available to overcome the neuromuscular blocker
effect at the nicotinic receptor, but also causing muscarinic stimulation
Neostigmine – shares duration of action with glycopyrrolate (see below)
Edrophonium – shares duration of action with atropine (see below)
Physostigmine – crosses the BBB, therefore useful for atropine overdose
Anticholinergics: given with reversal agents to block the muscarinic effects
of cholinergic stimulation, also excellent for treating bradycardia and excess
secretions
Atropine – used in conjunction with edrophonium, crosses the BBB causing
drowsiness, so maybe bad at end of surgery for reversal, some use as
premed for all children since they tend to become bradycardic with
intubation and produce copious drool
Glycopyrrolate – used in conjunction with neostigmine, does not cross the
BBB
Commonly Used Medications
Questions?
Thank you for listening.
Editor's Notes
#1 Local and regional anesthesia and analgesia techniques depend on a group of drugs — local anesthetics — that transiently inhibit some or all of sensory, motor, or autonomic nerve function when the drugs are applied near neural tissue. This lecture presents the mechanism of action, structure–activity relationships, clinical pharmacology of local anesthetic drugs and some methods of use such medications in anesthesiology
#2 It has been recognized for many years that some naturally occurring substances can produce local or generalized changes in sensory appreciation and motor power.
The naturally occurring alkaloid cocaine was the first local anaesthetic used in clinical practice.
It is derived from a shrub (Erythroxylon coca) that grows in the foothills of the Andes, and for many centuries its leaves were chewed by Peruvian Indians for its mood elevating and stimulant properties.
Pure cocaine was first isolated by Niemann in 1860, who confirmed its effects on sensation,
Its pharmacological actions were studied by Von Anrep between 1870 and 1880.
The drug was introduced into clinical practice by Freud and K¨oller in 1884.
Sigmund Freud used cocaine in an attempt to treat a morphine-dependent colleague, but instead converted him into a cocaine addict.
#3 Karl K¨oller initially used cocaine to produce corneal anaesthesia in experimental animals and rapidly appreciated its potential advantages. He introduced it into ophthalmological practice as a surface anaesthetic, and its use for infiltration, conduction and spinal anaesthesia soon followed.
Unfortunately, its potential for producing drug dependence was not initially appreciated.
Nevertheless, by 1890, its dangers were well recognized, and a search began for newer and safer drugs.
Procaine, the first synthetic local anaesthetic, was introduced by Alfred Einhorn in 1905.
Many other synthetic local anaesthetic esters were subsequently investigated. Most of these have now been discarded and are solely of historical interest. However, the local anaesthetic ester tetracaine is still widely used to produce topical anaesthesia.
#4 An important milestone occurred in 1943 when lidocaine was synthesized by Lofgren and subsequently introduced into anaesthetic practice.
This aminoacylamide was the prototype of a new group of local anaesthetic drugs.
Since the advent of lidocaine, other amides have been introduced, some of which have been developed as single stereoisomers with significant clinical advantages.
#5 Peripheral nerves consist of the dendrites and axons of sensory and/or motor nerves, which are bound together and surrounded by connective tissue. Layers of longitudinally arranged collagen surround individual nerve fibres (the endoneurium) or groups of nerve fibres (the perineurium). An outer connective tissue sheath (the epineurium) surrounds the nerve trunk and carries its blood vessels and lymphatics. Each nerve fibre is connected with a central cell body from which it receives its metabolic and nutritional requirements and is surrounded by a sheath of Schwann cell cytoplasm.
#6 Unmyelinated fibres are usually enclosed in groups by the sheath of a single Schwann cell which is in contact with the cytoplasm of adjacent Schwann cells.
In contrast, each myelinated fibre is enclosed by the cytoplasm of a single Schwann cell, with its phospholipid cell membrane wound spirally around the fibre to form the myelin sheath.
Between individual Schwann cells the myelin sheath is absent, and the resultant junctions between adjacent cells are known as the nodes of Ranvier. The internodal distance is related to the size of the Schwann cells and the diameter of the nerve fibres. In large myelinated nerves, the intermodal distance may be 1–2 mm.
#7 Individual nervefibres consist of a central core (the neuroplasm), which is enclosed by a limiting cell membrane (the neurilemma). The neuroplasm contains mitochondria, microtubules and neurofilaments, whichare required for normal nutrition and metabolism.
In contrast, the neurilemma is a characteristic phospholipid membrane and contains integral proteins (Fig. 1.1). Some of these proteins contain pores or ion channels, which play an important role in neuronal function.
#8 Excitable cells (eg, neurons or cardiac myocytes) have the unusual capability of generating action potentials. Membrane-associated, voltage-gated Na channels in peripheral nerve axons can produce and transmit membrane depolarizations following chemical, mechanical, or electrical stimuli.
Activation of voltage-gated Na channels causes a very brief (roughly 1 ms) change in the conformation of the channel, allowing an influx of Na ions and generating an action potential The increase in Na permeability causes temporary depolarization of the membrane potential to +35 mV. The Na current is brief and is terminated by inactivation of voltage-gated Na channels, which do not conduct Na ions. When there is no Na ion flux the membrane returns to its resting potential.
When a stimulus is sufficient to depolarize a patch of membrane, the signal can be transmitted as a wave of depolarization along the nerve membrane (an impulse). Baseline concentration gradients are maintained by the sodium–potassium pump, and only a minuscule number of Na ions pass into the cell during an action potential.
#9 Neurons (and all other living cells) maintain a resting membrane potential of −60 to −70 mV. The electrogenic, energy-consuming sodium–potassium pump (Na+- K+-ATPase) couples the transport of three sodium (Na) ions out of the cell for every two potassium (K) ions it moves into the cell. This creates a concentration gradient that favors the movement of K ions from an intracellular to an extracellular location, and the movement of Na ions in the opposite direction.
The cell membrane is normally much more “leaky” to K ions than to Na ions, so a relative excess of negatively charged ions (anions) accumulates intracellularly. This accounts for the negative resting membrane potential
Action potential propagates along the axon unidirectionally. The upstream region of the axonal membrane is still in the refractory period and unable to achieve the threshold for depolarization.
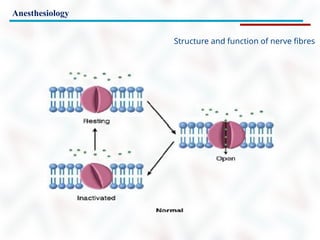
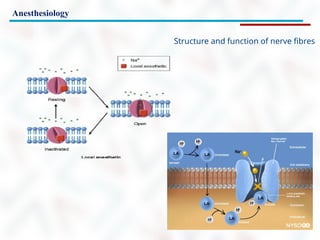
#10 The previously mentioned, voltage-gated Na channels are membrane-associated proteins comprising one large α subunit, through which Na ions pass, and one or two smaller β subunits. Na channels exist in (at least) three states —resting (nonconducting), open (conducting), and inactivated (nonconducting)
#11 When local anesthetics bind a specific region of the α subunit, they prevent channel activation and Na influx through the individual channels. Local anesthetic binding to Na channels does not alter the resting membrane potential.
With increasing local anesthetic concentrations, an increasing fraction of the Na channels in the membrane bind a local anesthetic molecule and cannot conduct Na ions. As a consequence of more channels binding a local anesthetic, the threshold for excitation and impulse conduction in the nerve increases, the rate of rise and the magnitude of the action potential decreases, and impulse conduction velocity slows.
At great enough local anesthetic concentrations (when a sufficient fraction of Na channels has bound a local anesthetic), action potentials can no longer be generated and impulse propagation is abolished
#12 Local anesthetics have a greater affinity for the Na channel in the open or inactivated state than in the resting state. Depolarizations lead to open and inactivated channels; therefore, depolarization favors local anesthetic binding.
The fraction of Na channels that bind a local anesthetic increases with frequent depolarization (eg, during trains of impulses). This phenomenon is termed use dependent block. Put another way, local anesthetic inhibition of Na channels is both voltage (membrane potential) and frequency dependent. Local anesthetic binding is greater when nerve fibers are firing and depolarizing frequently than with infrequent depolarizations.
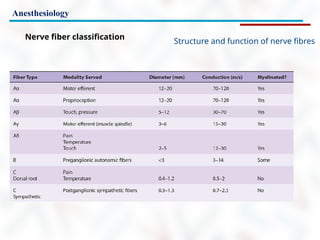
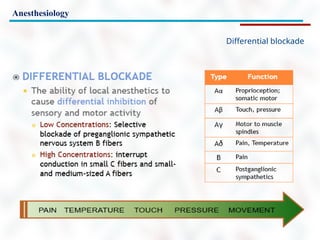
#13 Sensitivity of nerve fibers to inhibition by local anesthetics is influenced by axonal diameter, myelination, and other factors. Table lists the most commonly used classification for nerve fibers.
In comparing nerve fibers of the same type (myelinated versus unmyelinated), smaller diameter associates with increased sensitivity to local anesthetics.
Thus, larger, faster-conducting Aα fibers are less sensitive to local anesthetics than smaller, slower-conducting Aδ fibers.
Larger unmyelinated fibers are less sensitive than smaller unmyelinated fibers.
On the other hand, small unmyelinated C fibers are relatively resistant to inhibition by local anesthetics as compared with larger myelinated fibers. In a human peripheral nerve the onset of local anesthetic inhibition generally follow this sequence: autonomic before sensory before motor. But at steady state, if sensory anesthesia is present, usually all modalities are inhibited.
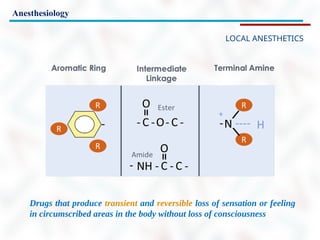
#14 All currently available local anesthetics consist of a lipophilic group (usually an aromatic benzene ring) separated from a hydrophilic group (usually a tertiary amine) by an intermediate chain that includes an ester or amide linkage.
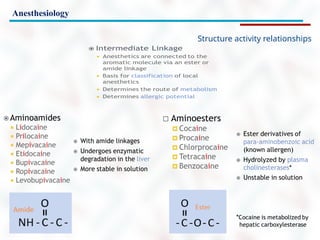
#15 Based on the nature of the intermediary chain, clinically used local anesthetics are classified as amino amides (e.g., lidocaine, prilocaine, bupivacaine) or amino esters (e.g., cocaine, procaine, chloroprocaine, tetracaine).
#16 Amide and ester local anesthetics differ in their chemical stability, metabolism, and allergic potential.
Amides are extremely stable, whereas esters are relatively unstable, particularly in neutral or alkaline solution.
Amide compounds undergo enzymatic degradation in the liver, whereas ester compounds are hydrolyzed in plasma by esterases.
Cocaine, an ester, is an exception, as it is metabolized predominantly by the liver.
#17 The major difference between ester- and amide-type local anesthetics is their metabolism.
Ester-type local anesthetics undergo hydrolysis by plasma esterases. An exception to this is cocaine, which is metabolized in the liver by carboxylesterase.
Amide-type local anesthetics undergo biotransformation mainly in the liver.
The metabolites of amide-type local anesthetics are excreted by the kidneys. About 5% of amide type local anesthetics is renally excreted unchanged.
Therefore patients with decreased hepatic or renal function eliminate amide-type local anesthetics more slowly and are at increased risk for systemic toxicity.
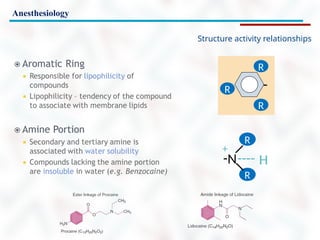
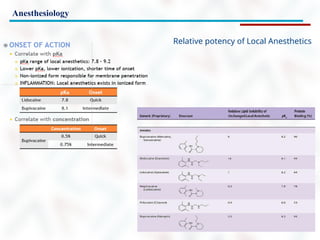
#18 Clinical local anesthetic potency correlates with octanol solubility and the ability of the local anesthetic molecule to permeate lipid membranes. Potency is increased by adding large alkyl groups to a parent molecule (compare tetracaine with procaine, or bupivacaine with mepivacaine).
On the other hand, whereas the correlation between local anesthetic potency and hydrophobicity generally holds true in vitro, it may not be as exact in vivo. As opposed to setups with isolated nerves, other factors may influence the potency of local anesthetics on nerves in situ.34 For example, highly lipid-soluble agents may be sequestered into surrounding adipose cells. Vasodilatory properties of local anesthetics may likewise alter drug redistribution into the neighboring tissues
There is no clinical measurement of local anesthetic potency that is analogous to the minimum alveolar concentration (MAC) of inhalation anesthetics. The minimum concentration of local anesthetic that will block nerve impulse conduction is affected by several factors, including fiber size, type, and myelination; pH (an acidic environment antagonizes clinical nerve block); frequency of nerve stimulation; and electrolyte concentrations (hypokalemia and hypercalcemia antagonize blockade).
#19 Onset of local anesthetic action depends on many factors, including lipid solubility and the relative concentration of the nonionized, more lipid-soluble free-base form (B) and the ionized water-soluble form BH+), expressed by the pKa. The pKa is the pH at which there is an equal fraction of ionized and nonionized drug. Less potent, less lipid-soluble agents (eg, lidocaine or mepivacaine) generally have a faster onset than more potent, more lipid-soluble agents (eg, ropivacaine or bupivacaine).
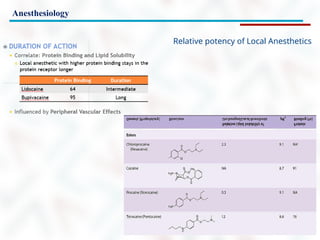
#20 Duration of action correlates with potency and lipid solubility. Highly lipidsoluble local anesthetics have a longer duration of action, presumably because they more slowly diffuse from a lipid-rich environment to the aqueous bloodstream. Lipid solubility of local anesthetics is correlated with plasma protein binding. In blood local anesthetics are mostly bound by α1-acid glycoprotein and to a lesser extent to albumin.
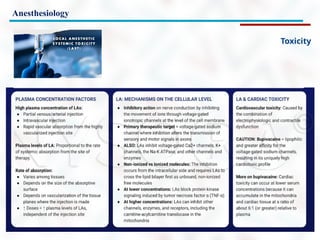
#22 It was assumed that only a very small fraction (1%-2%) of local anesthetic reaches the nerve membrane even when placed in close proximity to the nerve.
With the advent of ultrasound-guided targeting, this fraction might be higher, but still a considerable amount of anesthetic is lost along the concentration gradient across different tissues. The quality of nerve blockade is determined by the potency, concentration, and volume of the local anesthetic.
The potency of a local anesthetic can be expressed as the minimum local anesthetic concentration at which complete nerve block is established.
The volume of local anesthetic is also important as a sufficient length of axon must be blocked to prevent regeneration of the impulse in the adjacent node of Ranvier.
This is understood by the phenomenon of decremental conduction, whereby depolarization of the membrane decays with the distance away from the front of the action potential, and impulse propagation stops when the depolarization falls below the conduction threshold.
If less than the critical length of the axon is blocked (usually assumed to be three nodes of Ranvier), the action potential can be regenerated in the proximal membrane segment or node when the decaying depolarization is still above threshold for Na+ channel activation
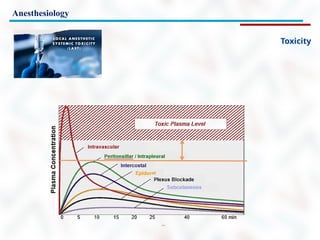
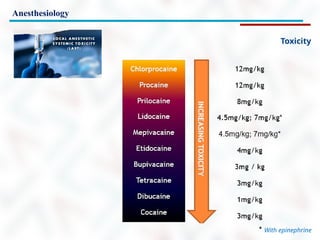
#23 The toxicity of local anesthetics is the main limiting factor in their clinical applications. Local anesthetics are relatively safe if administered appropriately. However, significant systemic or localized toxicity can result from unintended intravascular, intrathecal, or intraneural injection or if excessive doses are administered, resulting in major systemic absorption
#24 Systemic Toxicity
The classic cascade of local anesthetic systemic toxicity (LAST) occurs after the administration of a relative overdose of local anesthetic—for example, for a peripheral nerve block, resulting in increased absorption into the systemic circulation and escalating symptoms.
These include CNS manifestations, followed by cardiovascular compromise. Other scenarios include inadvertent intravascular injection of local anesthetics, which can cause immediate cardiovascular collapse, and intraarterial injection during neck blocks that causes a short-lived seizure as local anesthetic directly enters the brain.
The initial symptoms depend on the plasma concentration of free local anesthetic and patient factors such as acidosis, protein binding, and comorbidities, and vary widely.
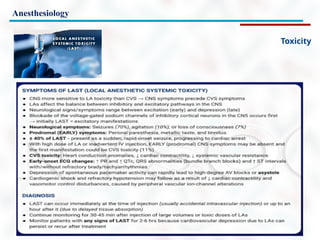
#25 The typical presentation of LAST usually begins with prodromal symptoms and signs, such as perioral numbness, tinnitus, agitation, dysarthria, and confusion.
These may be followed by more severe central nervous system derangements such as seizures and coma.
CardioVascular derangements can occur as well, initially presenting with hypertension and tachycardia, then bradycardia and hypotension, with progression to more serious complications, including ventricular arrhythmias and asystole.
The majority of adverse events occur within 1 minute after injection of LA, but not all cases follow this pattern. Toxicity can have a delayed onset, of greater than 1 hour after injection, and can manifest as isolated CV dysfunction or as a combination of CNS and CardioVascular signs without the classical progression
Variables that increase the risk of toxicity include the type of LA and dose, site of injection, the patient’s comorbidities, extremes of age, and small size or limited muscle mass. The lipophilicity of a LA is associated with toxicity. More lipophilic LAs like bupivacaine have an increased risk of toxicity relative to the less-lipophilic LAs like mepivacaine and lidocaine.
Higher total dose and the dose-to-weight ratio of the drug can potentially increase the possibility of LAST.
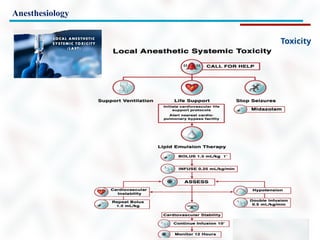
#26 Presently, the three pillars of LAST treatment consist of seizure management, advanced cardiac life support (ACLS), and prompt administration of a 20% lipid emulsion.
For hemodynamically stable patients with isolated seizure activity, intravenous benzodiazepines may be used.
Small doses of propofol are considered by some an acceptable alternative for seizure control but can worsen cardiac dysfunction that may develop with LAST.
Supplemental oxygen is appropriate for any patient exhibiting signs of LAST, but for patients with apnea, hemodynamically unstable arrhythmias, or cardiac arrest, immediate, more aggressive airway management or circulatory support is required. The goals are to maintain pulmonary ventilation and adequate organ perfusion with well-oxygenated blood and to avoid further acidosis until initiation of lipid emulsion therapy.
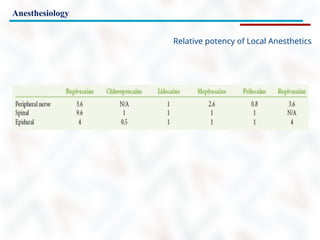
#27 The slide shows relative toxicity of local anesthetics
#28 So the definitions are pretty straightforward, actually.
The injection of local anesthetics into areas to produce anesthesia sufficient for surgical procedures to be performed without discomfort to the patient. That's regional anesthesia.
And that's typical of subarachnoid block or spinal block. It's also typical of what we see with epidural blocks.
With peripheral nerve blocks, it's never quite as clear as that.
We certainly can produce can do surgery with some of these blocks, but in many cases the blocks are inadequate for surgical anesthesia but produce excellent post-operative analgesia.
So regional analgesia is the injection of the same local anesthetic into areas of the body to produce analgesia for postoperative pain relief.
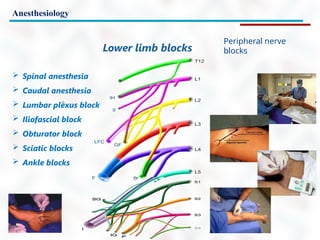
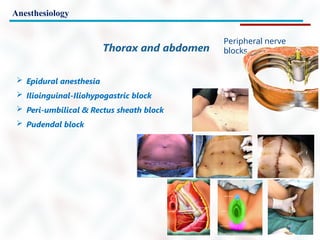
#31 Spinal anesthesia provides excellent operating conditions for surgery below the umbilicus. Thus, it has been used in the fields of urological, gynecological, obstetric, and lower abdominal and perineal general surgery. Likewise, it has been used in lower limb vascular and orthopedic surgery
#36 So what's the difference between an epidural and a spinal? Well, the big difference is three millimeters. And it's a very small distance when you're putting pressure on the back and you can feel the needle moving forward. But the difference in block is quite profound.
Epidurals produce good anesthesia but not profound anesthesia. So patients with an epidural block will feel pressure when the when the surgeon pushes on their abdomen may feel position changes as the surgeon moves back and forth and may have some sense of work going on.
It's a very good technique for patients in labor, because you can use it for an extended period of time, because a catheter is placed and you can give very dilute local anesthetics over a period of time that cause excellent labor pain relief. And then if you have to, you can change it to an anesthetic for surgical pain. You could adjust the rate of flow through the catheter. You can adjust the dose and strength of the local anesthetic that's being used to modify your block to the patient's needs
In the case of a spinal, the first thing is that when you get into the spinal space, the subarachnoid space, you're actually in the central nervous system.
You do not place a catheter in this situation. You merely inject local anesthetic, sometimes with very dilute morphine or other narcotic into the space. You get a very profound block. The patients have absolutely no sensation below the waist with this block.
Those sensations of pressure or movement that I described for the epidural are absent in the case of a spinal. And for the ideal surgical situation, a spinal is actually superior to an epidural. The negative about a spinal is you can't adjust it. You can't decrease or change the flow of the drug. It's a one shot technique.
#37 The needles we use for spinal now are very small needles. They actually have to be put through an introducer.
The one on the right is called a Quanqi needle, and this is an old fashioned needle. Although we still use it in some situations.
They tended to be larger needles, but you can see that the tip of the needle is sharp, and that whole area around the hole in the needle tip is a cutting edge, and it'll cut through tissues very easily.
The problem with this needle is that it caused holes that were big enough for cerebral spinal to fluid to continue to leak out of the central nervous system after the block was in place, and this could lead to extremely severe headaches, which were sometimes quite difficult to treat.
About 20 years ago, a new type of needle was introduced and this was the Sprott Needle. And that's the one center of this diagram. And you can see that the tip is different. It's a pencil point tip. It has no cutting edge. It basically forces its way between the fibers of the ligaments without cutting them.
The hole on this needle is not right at the tip. It's down a little bit down the shaft. And in the Sprott Needle it was a very big hole. And that became a problem because it was possible to have a portion of the hole in the subarachnoid space and a portion of it outside the subarachnoid space, so that when you injected the local anesthetic, some of it would go into the right place, but some of it would just get lost.
The needles we use now are the ones that I use now are called Whitaker Needles, and they're very similar to the Sprott, except the hole is much smaller and much closer to the tip, and the chances of injecting local anesthetic into the wrong space is largely eliminated.
#38 Typically 17–18 gauge
9cm to hub
Tuohy needle most commonly used
Blunt bevel with a gentle curve of
15–30° at the tip
Pushes away the dura after passing through the ligamentum flavum instead of penetrating it
Straight needles without a curved tip (Crawford needles) may have a higher incidence of dural puncture but facilitate passage of an epidural catheter.
Needle modifications include winged tips and introducer devices set into the hub designed for guiding catheter placement.
#40
Complication rate for "kiddie caudals" is very low
Total spinal and IV injection causing seizure or cardiac arrest
Intraosseous injection has also been reported to cause systemic toxicity
Calcification of the sacrococcygeal ligament may make caudal
anesthesia difficult or impossible
in older adults
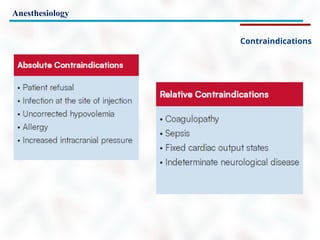
#41 Coagulopathy, previously considered an absolute contraindication, may be considered depending on the level of derangement.
Another relative contraindication of spinal anesthesia is sepsis distinct from the anatomic site of puncture (eg, chorioamnionitis or lower extremity infection). If the patient is on antibiotics and the vital signs are stable, spinal anesthesia may be considered.
Spinal anesthesia is relatively contraindicated in cardiac diseases with fixed cardiac output (CO) states. Aortic stenosis, once considered to be an absolute contraindication for spinal anesthesia, does not always preclude a carefully conducted spinal anesthetic
Indeterminate neurological disease is a relative contraindication. Multiple sclerosis and other demyelinating diseases are challenging.
In vitro experiments suggest that demyelinated nerves are more susceptible to local anesthetic toxicity. However, no clinical study has convincingly demonstrated that spinal anesthesia worsens such neurologic diseases. Indeed, with the knowledge that pain, stress, fever, and fatigue exacerbate these diseases, a stress-free central neuraxial nerve block (CNB) may be preferred for surgery.
Previous spinal surgery was once thought to be a contraindication. Dural puncture may be difficult, and spread of local anesthetic may be restricted by scar tissue. However, there are case reports of successful spinal anesthesia in this setting, particularly with the assistance of ultrasound.
#42
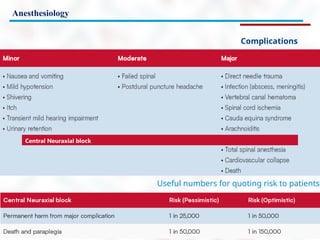
Cauda Equina Syndrome Cauda equina syndrome (CES) has been reported with the use of continuous spinal microcatheters. The use of hyperbaric 5% lidocaine for spinal anesthesia is associated with an increased incidence of CES, although other local anesthetics have been implicated.
#44 Requirements: no disruption of the venous system of the involved upper extremity because the technique relies on an intact venous system
Safety and efficacy depend on the interruption of blood flow into the involved limb and gradual release of the occluding tourniquet
Functions of tourniquet
Isolates the limb from systemic circulation (prevention of blood loss)
Isolates the systemic circulation from the limb (in IVRA)
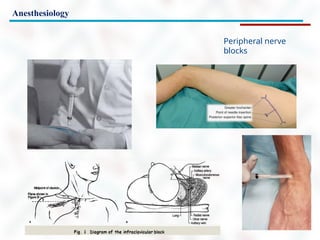
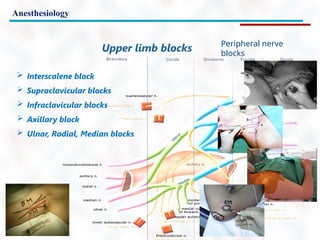
#46 There are many other regional blocks and virtually every portion of a limb, head or trunk can be blocked using a regional technique.
It's possible to do multiple blocks on the upper limb and multiple blocks on the lower limb the way we used to do this, the way I was taught to do it was to feel for an artery at the assumption being that the nerves to a certain area were closely in contact with that artery, passed the needle towards the artery until the patient complained of an electric shock going down their arm or down their leg.
The problem was that it failed a lot of the time, and if you actually got too close to the nerve and pierced the nerve causing that paraesthesia, that electric shock feeling you could actually damage the nerve, and because we weren't seeing where the needle tip was going, even though we were trying not to hit the artery that we were palpating.
At the same time, it wasn't unusual to hit the artery and for hematoma to form in the area,
#47 For the past 20 years the use of a nerve simulator to identify the nerve position has been popular and successful, but still not as perfect as one would wish.
With a nerve simulator you start with a current through isolated needle and advance towards the nerve and you watch the patient's muscles to see if there's a twitch that goes along with the nerve you're trying to block.
The whole procedure is blind other than the fact that you're putting a current in and you can see some movements in the limb.
You can't actually see the position of the nerve. You can't see the position of any arteries that might be in the area.
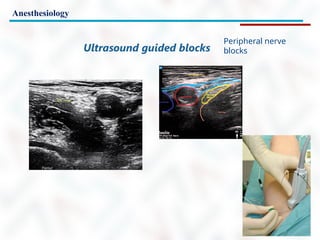
#50 Over the past 15 years the technique developed by Vincent Chan in Toronto has been widely accepted by anesthesiologists and this has really changed the situation.
This is called ultrasound guided needle placement and basically what it is using ultrasound to identify vessels and nerves and then passing a needle through tissue, watching the needle with the ultrasound until you're very close to the nerve and then injecting the local anesthetic at the nerve and you can see all this using the ultrasound.
#51 Now we'll watch a video on ultrasound guided femoral nerve block.
#54 So in summary, in this talk, we've talked about regional anaesthesia and analgesia. We've spent some time discussing epidural and spinal anesthesia neuraxial blocks and how they can be used for surgery or in the case of epidurals, how it can be used for labor analgesia or for postoperative pain control. We've talked about various methods by which peripheral nerves can be blocked, with emphasis on ultrasound guided techniques that have higher efficacy and lower complication rates.

![Anesthesiology
Ionic (sodium ion [Na+]) currents measured by voltage-clamp technique by depolarization
applied infrequently (“tonic” test). After equilibration with 0.2 mM lidocaine, the currents measured tonically
are reduced significantly compared with control currents. Application of repeate depolarizations results in a
dynamic reduction of currents after each depolarization (use-dependent inhibition).
Modified from Butterworth JF, Strichartz GR. Molecular mechanisms of local anesthesia: a review
Anesthesiology 1990;72:711–734.
Structure and function of nerve fibres](https://image.slidesharecdn.com/12anesthesia3-250914080919-9ec1fb99/85/Presentation-for-a-lecture-on_Anesthesia_part_3-pptx-12-320.jpg)











































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
















