Downloaded 170 times
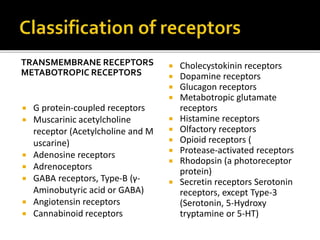
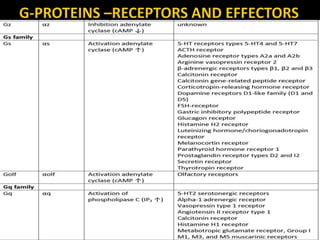
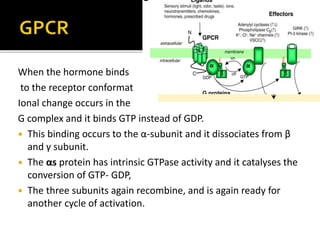
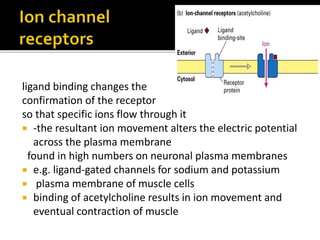
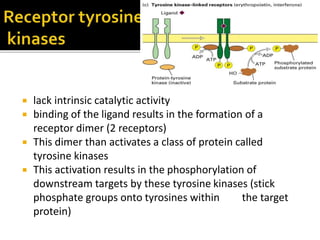
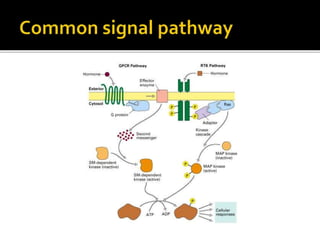
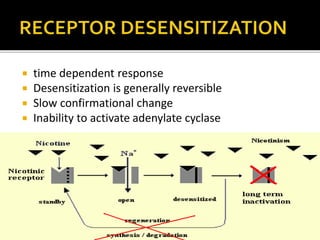
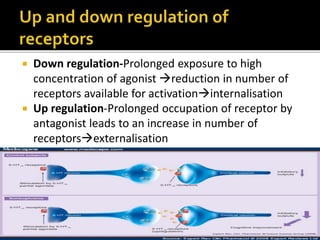
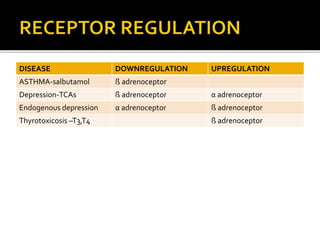
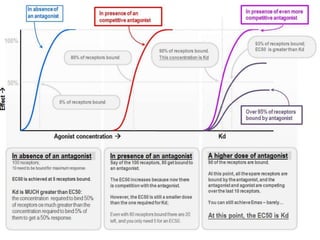


The document discusses different types of receptors and how they function. It describes transmembrane receptors like G protein-coupled receptors and ionotropic receptors. It also discusses intracellular receptors like nuclear receptors and receptor tyrosine kinases. The key concepts covered are how ligands bind to receptors and the downstream cell signaling pathways that are activated, including G proteins, second messengers like cAMP and IP3/DAG, and transcriptional regulation. Receptor properties like affinity, efficacy, desensitization, and regulation are also summarized.





































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





