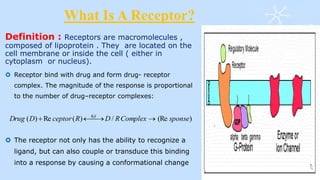
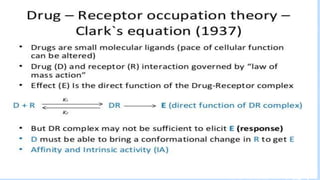
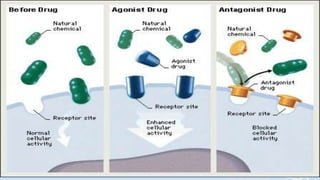
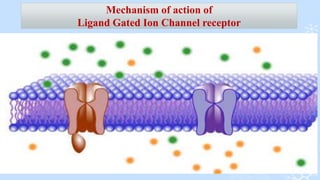
This document provides information about a receptor pharmacology course taught by Professor Dr. Md. Shah Amran at the University of Dhaka. It was prepared by 5 students and contains an introduction to receptors, classifications of different receptor types including ligand gated ion channels, G-protein coupled receptors, enzyme linked receptors, and nuclear receptors. It also discusses receptor-drug interactions, affinity, intrinsic activity, and mechanisms of cell surface and intracellular receptors.