Downloaded 464 times
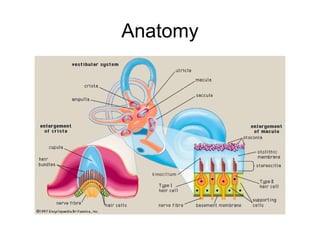
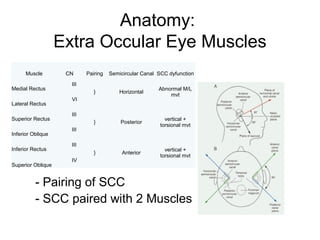
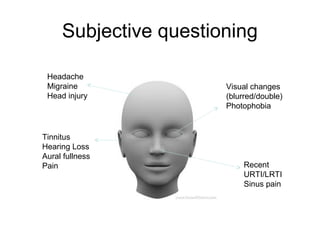
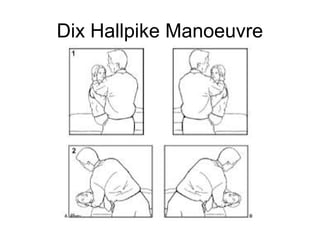
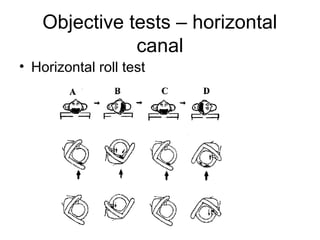

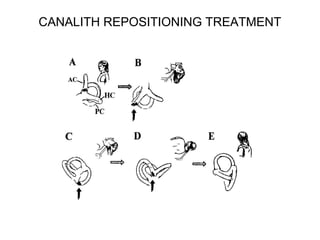
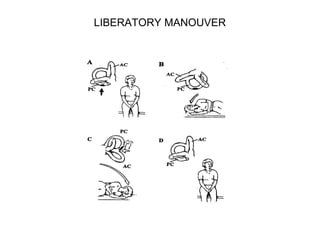
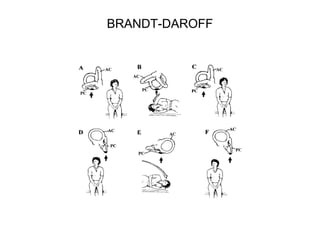
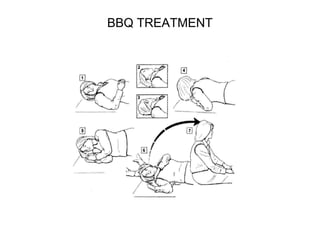
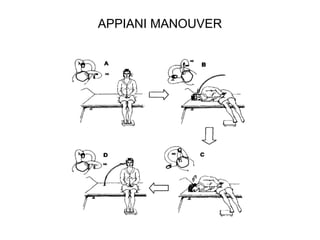
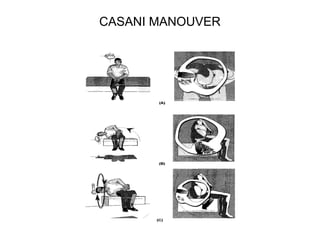

This document discusses vestibular assessment from a physiotherapy perspective. It begins with anatomy of the extraocular eye muscles and semicircular canals. Vestibular dysfunction can cause vertigo and imbalance, and the cause may be central or peripheral. A subjective history focuses on symptoms, tempo, and circumstances. Objective assessment includes eye movement testing, cerebellar tests, Rhomberg testing, and gait observation. Specific tests like Dix-Hallpike and roll tests evaluate the semicircular canals. Differential diagnoses and treatments like canalith repositioning maneuvers are also reviewed.











































































































