Downloaded 1,221 times

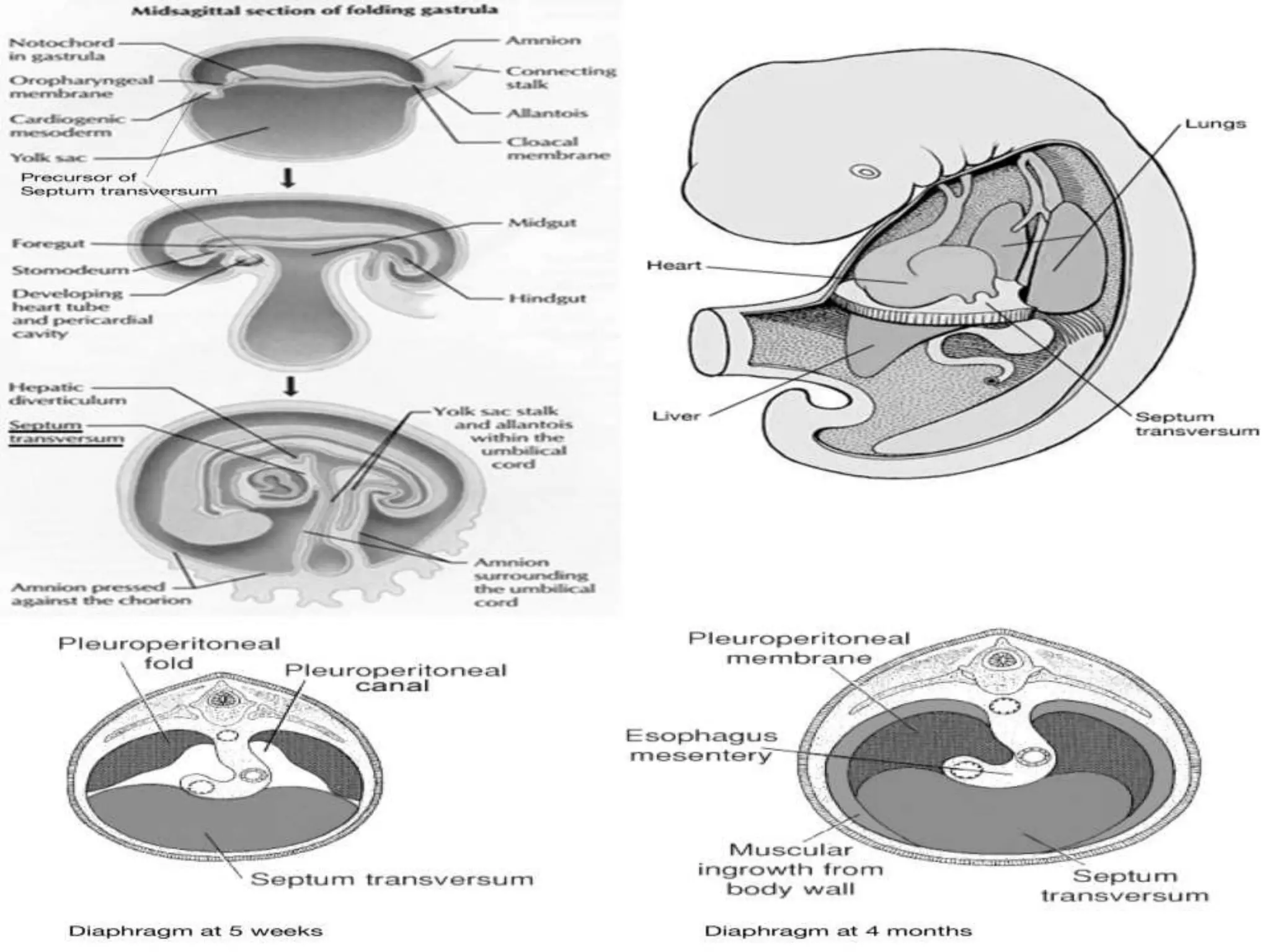
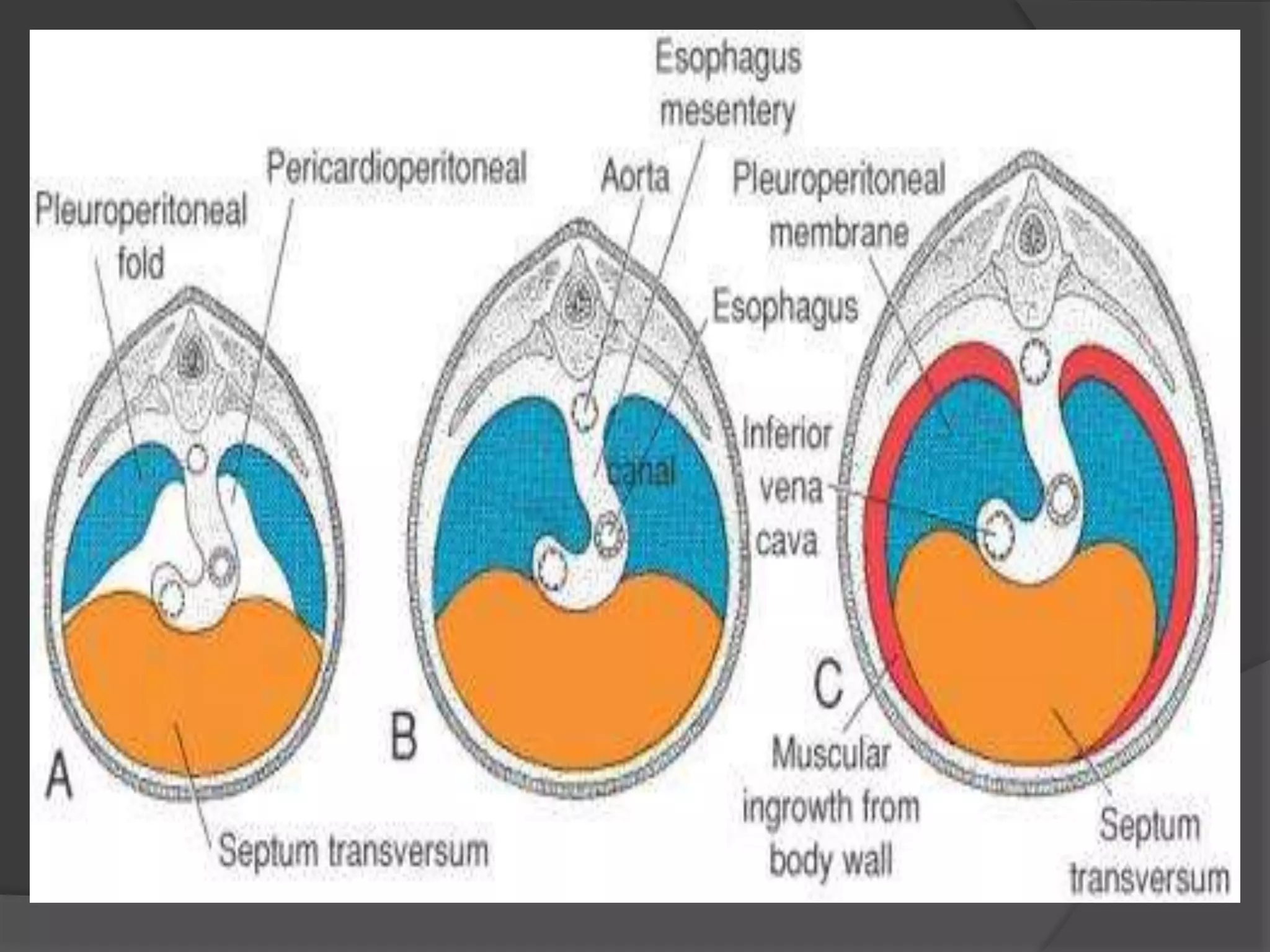





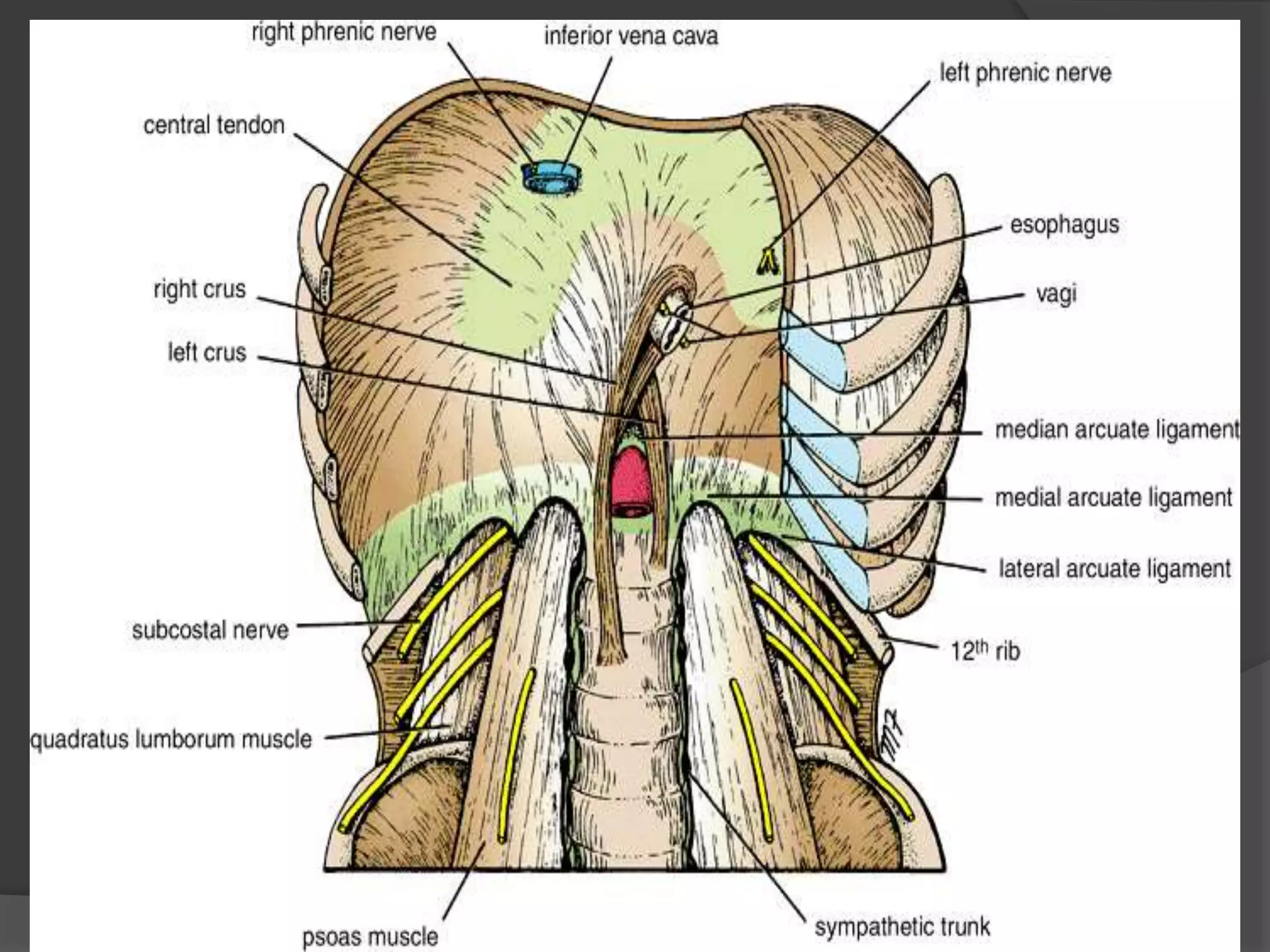



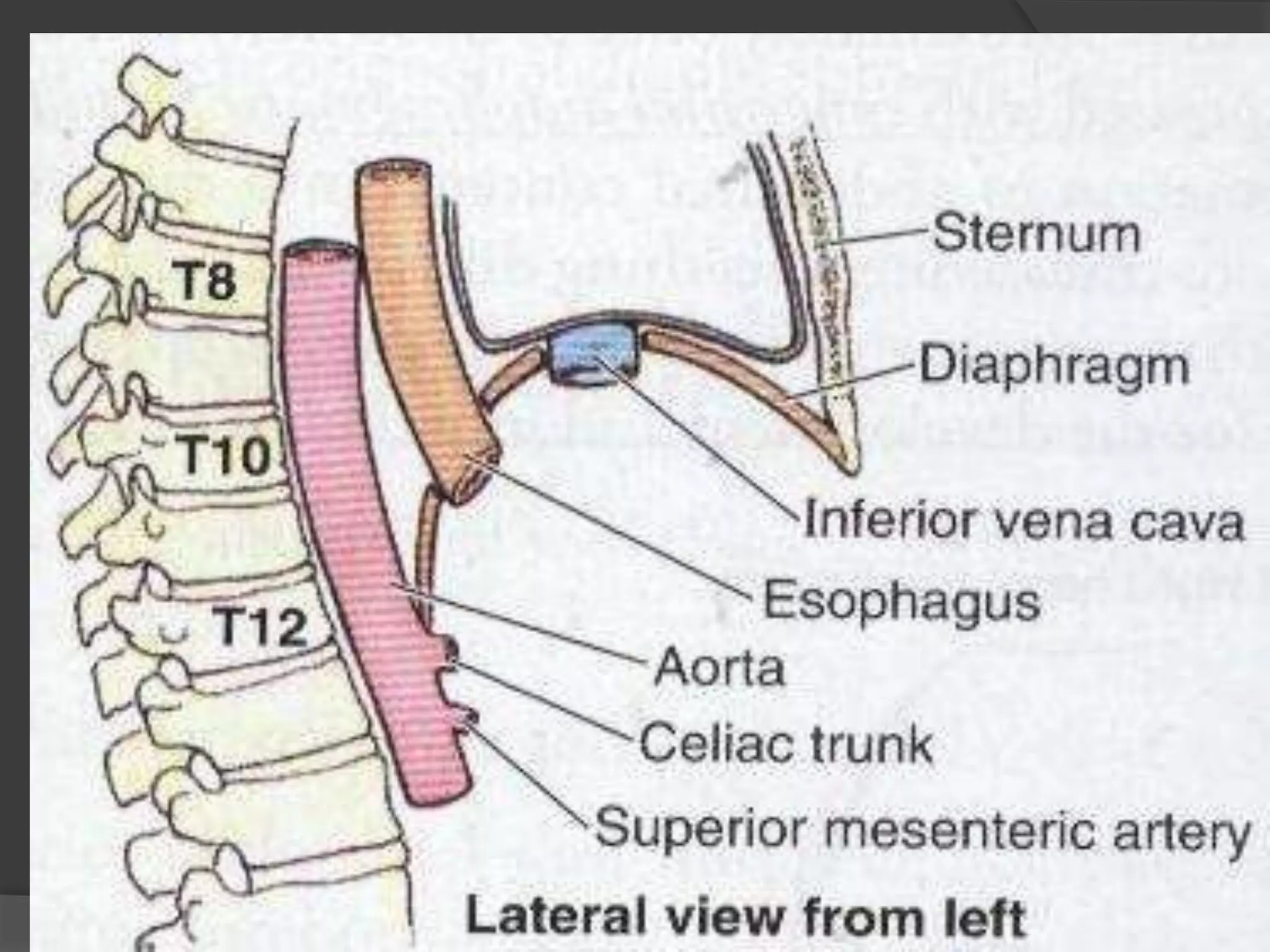
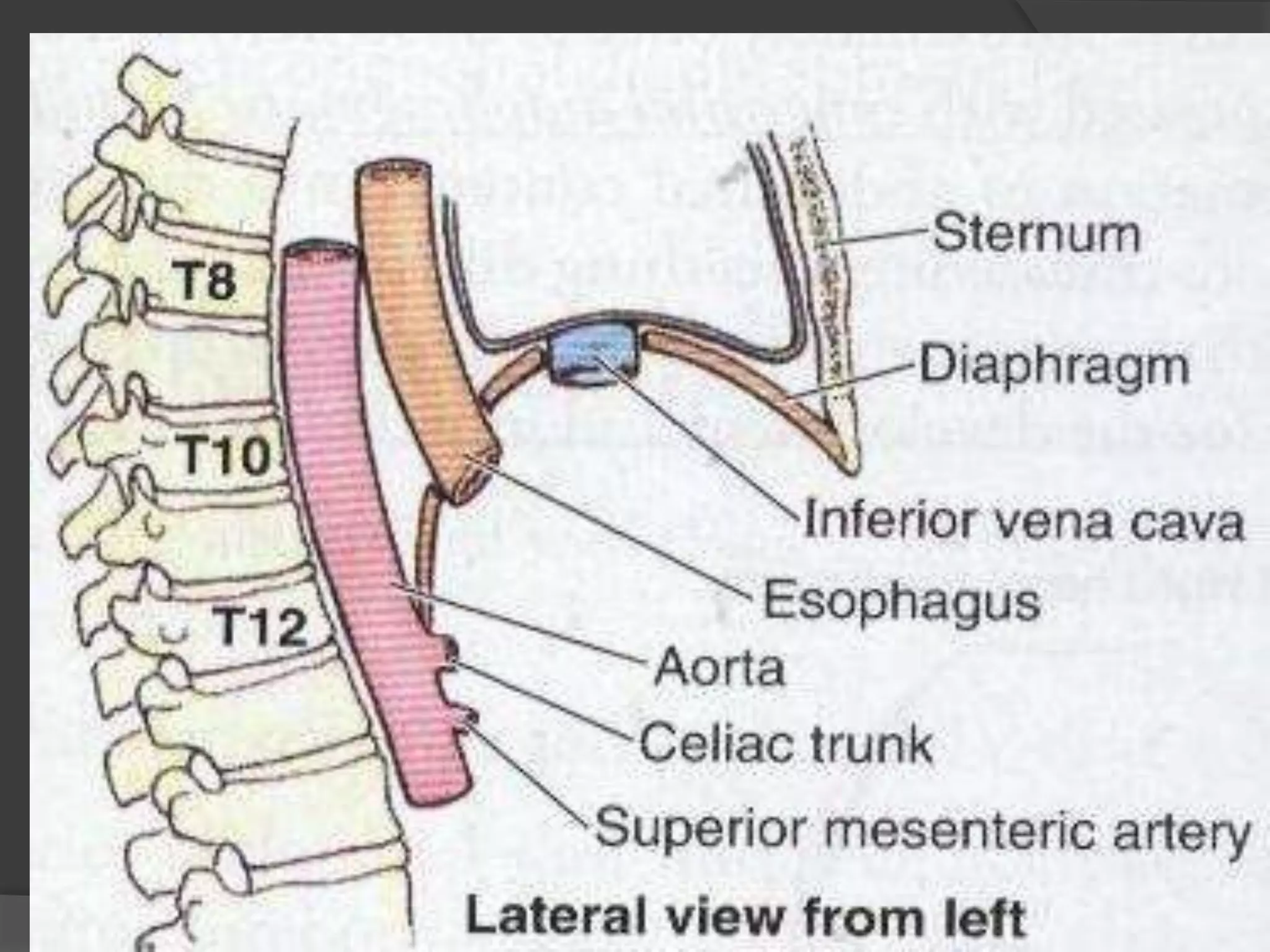
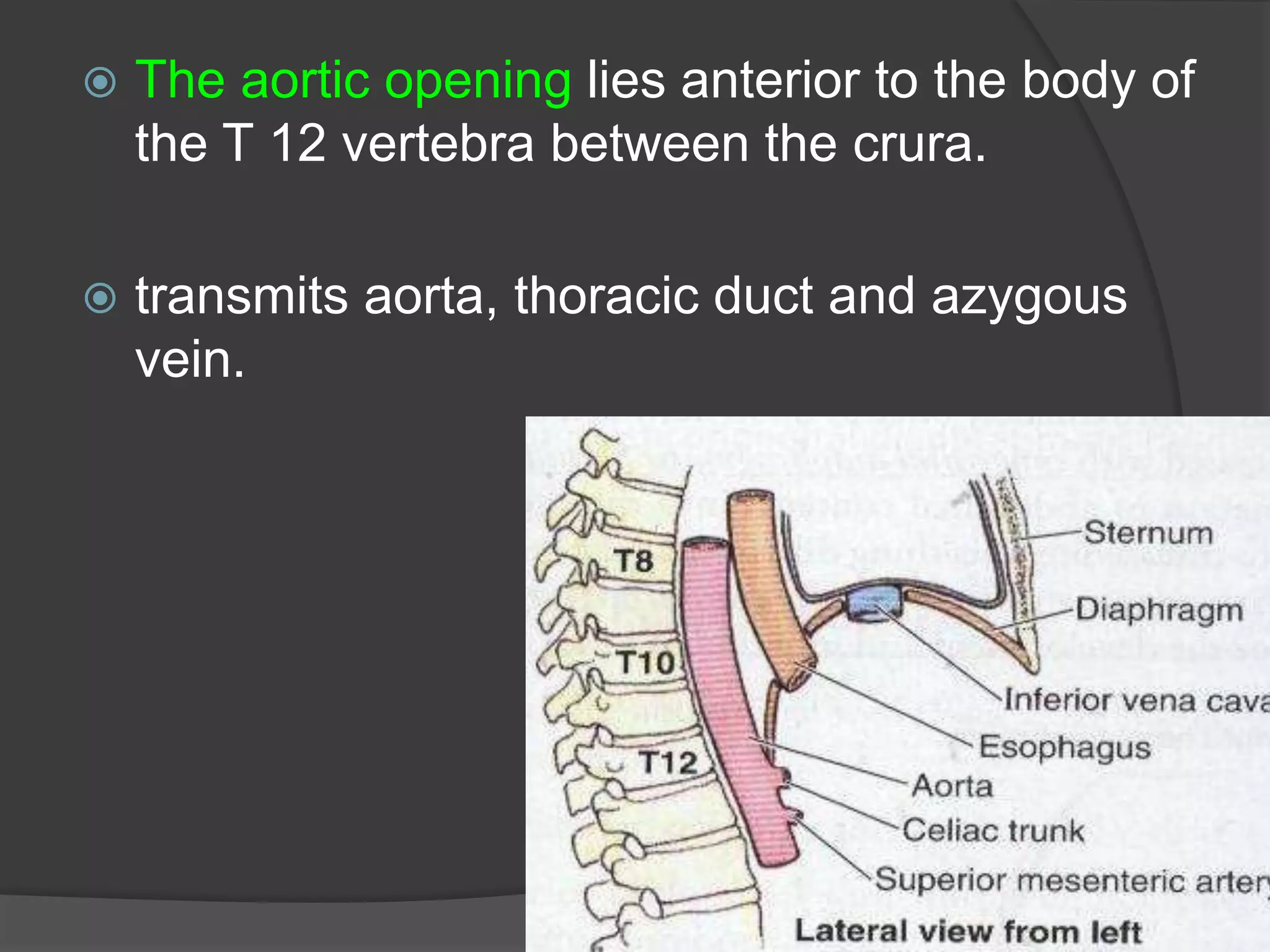



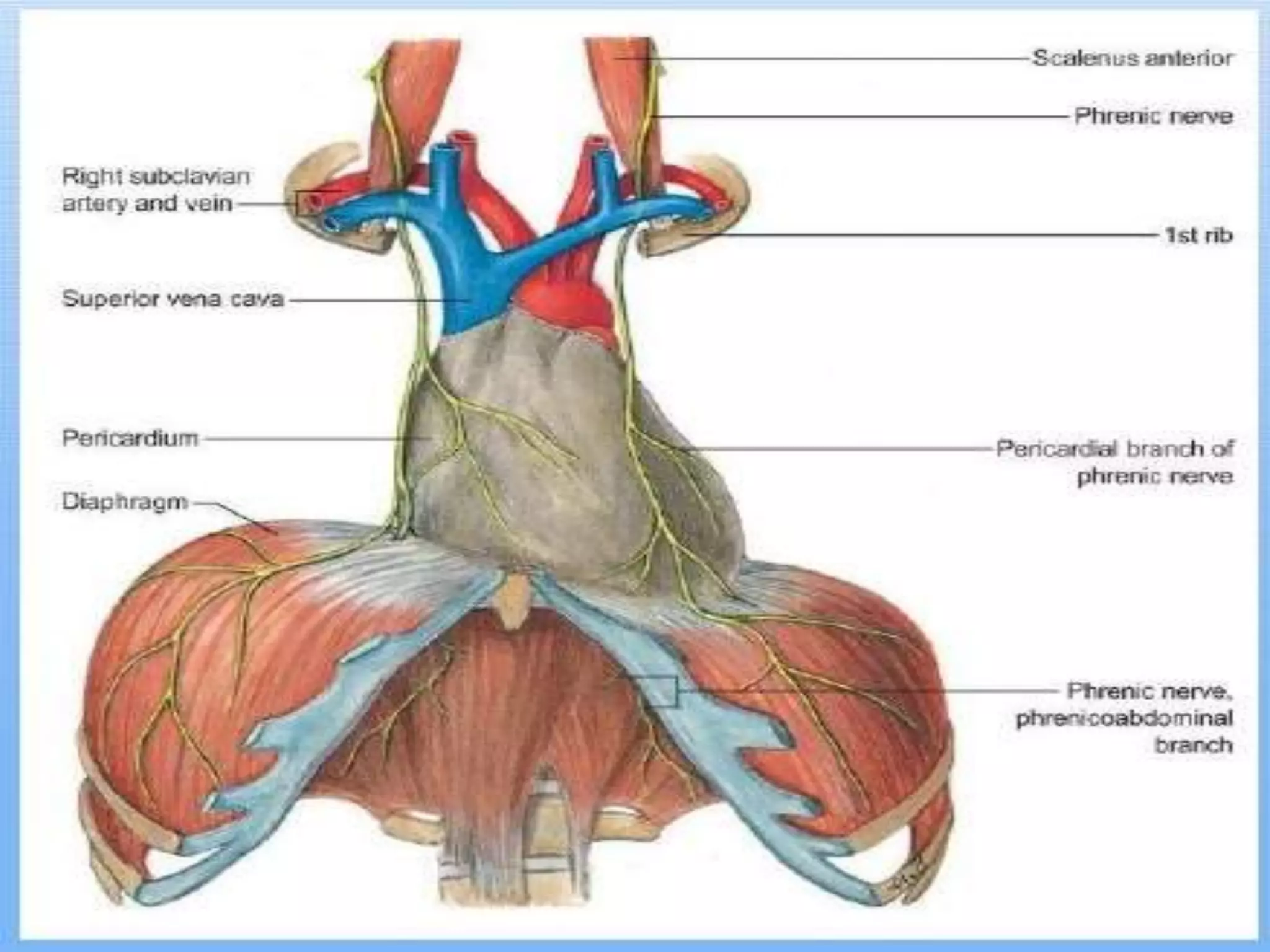

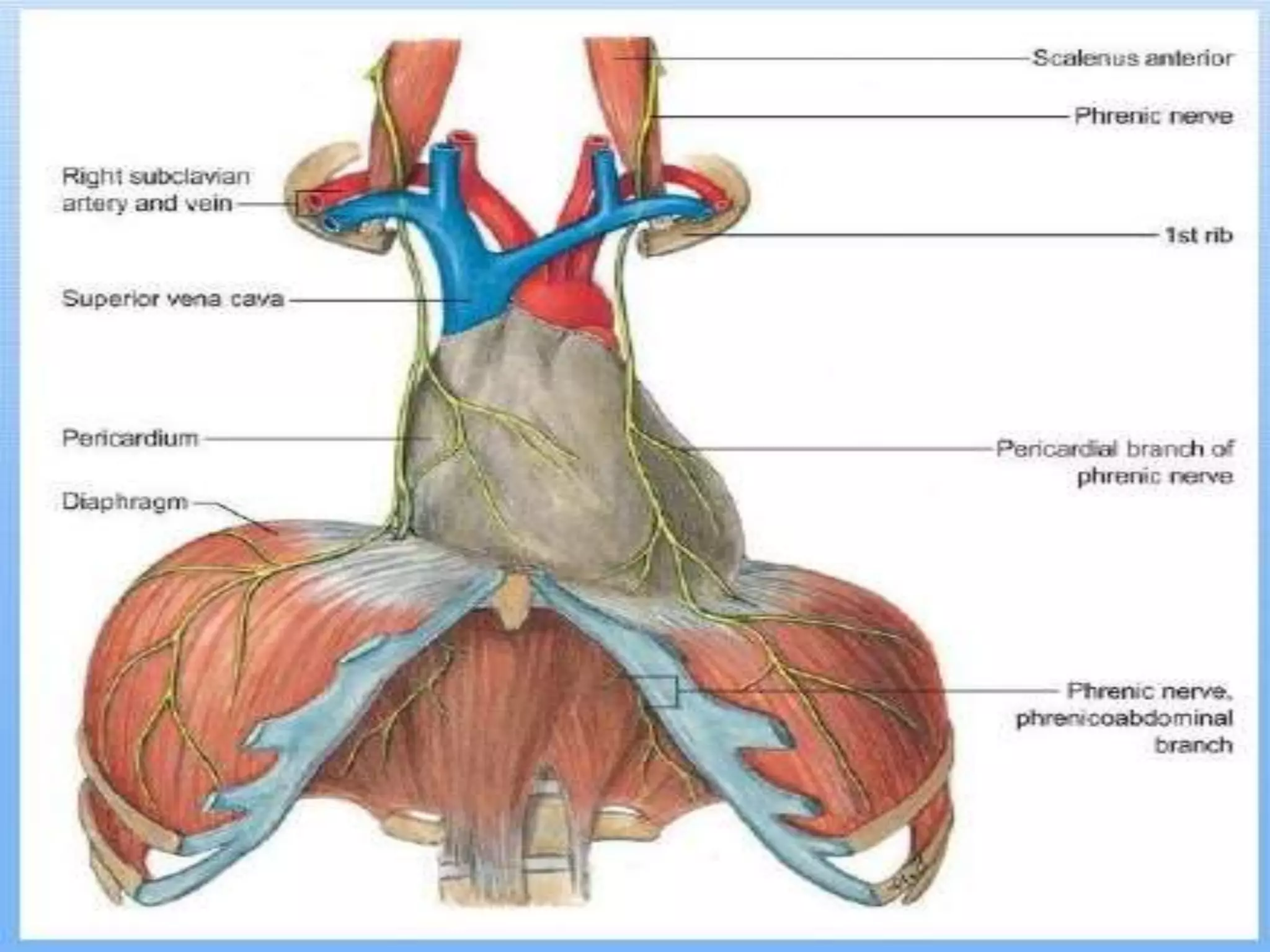


The diaphragm develops from four sources in the embryo and matures to become a dome-shaped musculofibrous sheet that separates the thoracic and abdominal cavities. It has a central tendon to which muscular fibers attach and is the primary muscle of respiration. During inspiration, it contracts to flatten and lower, increasing the vertical space in the thorax. It has openings that allow structures like the esophagus, inferior vena cava and aorta to pass between the thorax and abdomen. The phrenic nerves provide motor innervation and allow the diaphragm to contract during breathing.


































































































