Downloaded 379 times


































![Horner syndrome may appear, reflecting damage to the sympathetic neurons in the intermediolateral cell column.Extension of the syrinxsyringobulbia.[4, 5] T dysphagia, nystagmus, pharyngeal and palatal weakness, asymmetric weakness and atrophy of the tongue, and loss of pain ,temperature in the distribution of the trigeminal nerve.Syringocephalus -rarely, the syrinx cavity can extend beyond the medulla in the brain stem into the centrumsemiovale .Lumbar syringomyelia -atrophy of the proximal and distal leg muscles with dissociated sensory loss in the lumbar and sacral dermatomes. Lower limb reflexes are reduced or absent. Impairment of sphincter function is common.](https://image.slidesharecdn.com/syringomyelia-111008144704-phpapp01/85/Syringomyelia-46-320.jpg)

![Neurogenicarthropathies (Charcot joint) –MC-shoulder [6] Scoliosis is seen sometimes.[7, 8]](https://image.slidesharecdn.com/syringomyelia-111008144704-phpapp01/85/Syringomyelia-49-320.jpg)













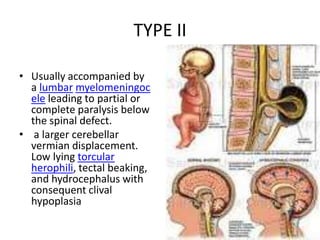
This document summarizes the medical history and examination findings of a 16-year-old male patient presenting with occipital headache, neck pain, loss of pain and temperature sensation in the left upper limb, and laxity of the left shoulder joint. Examination revealed loss of sensation from C3 to T2 on the left side and absent biceps and supinator reflexes on the left. MRI showed Arnold-Chiari malformation type 1 with syringomyelia involving the cervical and thoracic spinal cord. The patient was diagnosed with syringomyelia related to Arnold-Chiari malformation.























































































