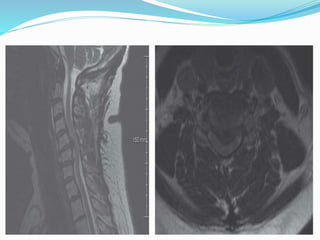
This document describes the medical history, examination, investigations, diagnosis, and treatment for a 53-year-old female patient presenting with neck pain and left arm weakness. She reported a 6-month history of neck pain radiating to both shoulders and arms, as well as recent proximal and distal weakness in her left arm. Her examination found increased tone and 4/5 weakness in her left arm. Imaging including X-ray, MRI, and CT of the cervical spine showed disc issues, spondylosis, and possible tumor. Her final diagnosis was cervical myelopathy. Her treatment included admission, counseling, optimization, surgery involving anterior cervical discectomy and fusion at three levels as well as two-level corpectomy, post