Downloaded 243 times

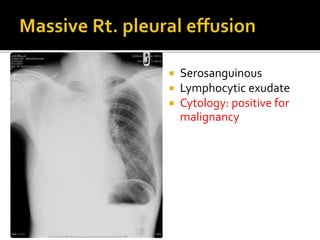

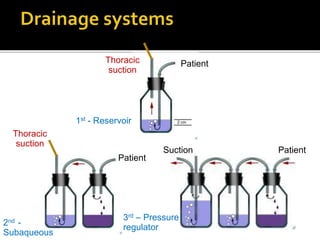
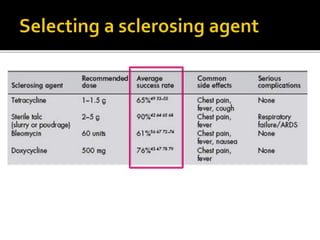







This document discusses the management of a 52-year-old man with stage IV lung cancer and a malignant pleural effusion. It provides guidelines for pleurodesis using sclerosing agents like tetracycline or talc to prevent further fluid accumulation. Complications, techniques, and management of failure are reviewed. Indications for different chest tube sizes and drainage systems are presented.























![Air leaks in Thoracic Surgery [Auto-saved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/airleaksinthoracicsurgeryauto-saved-230219163120-6180857a-thumbnail.jpg?width=640&height=640&fit=bounds)































































