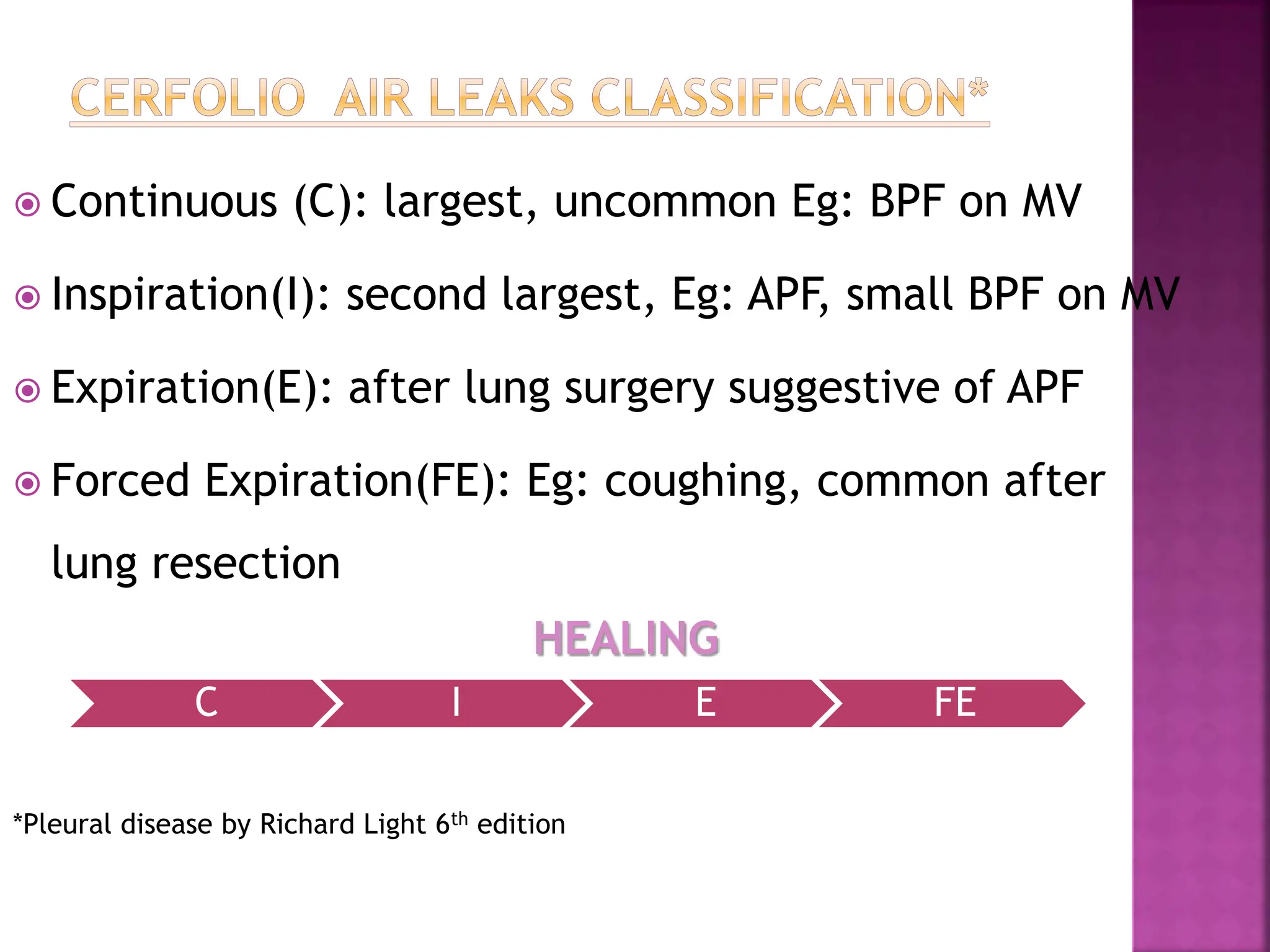
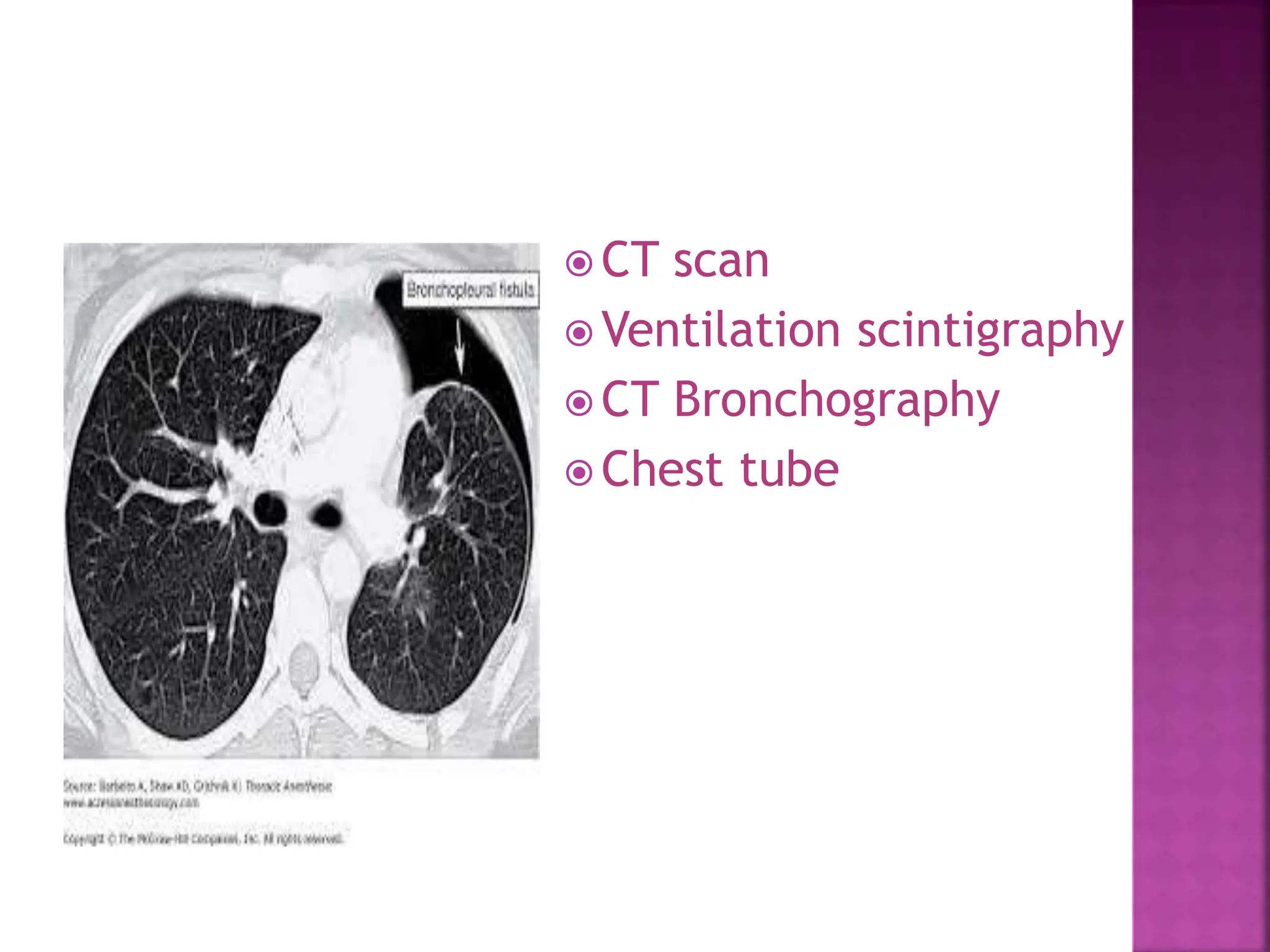
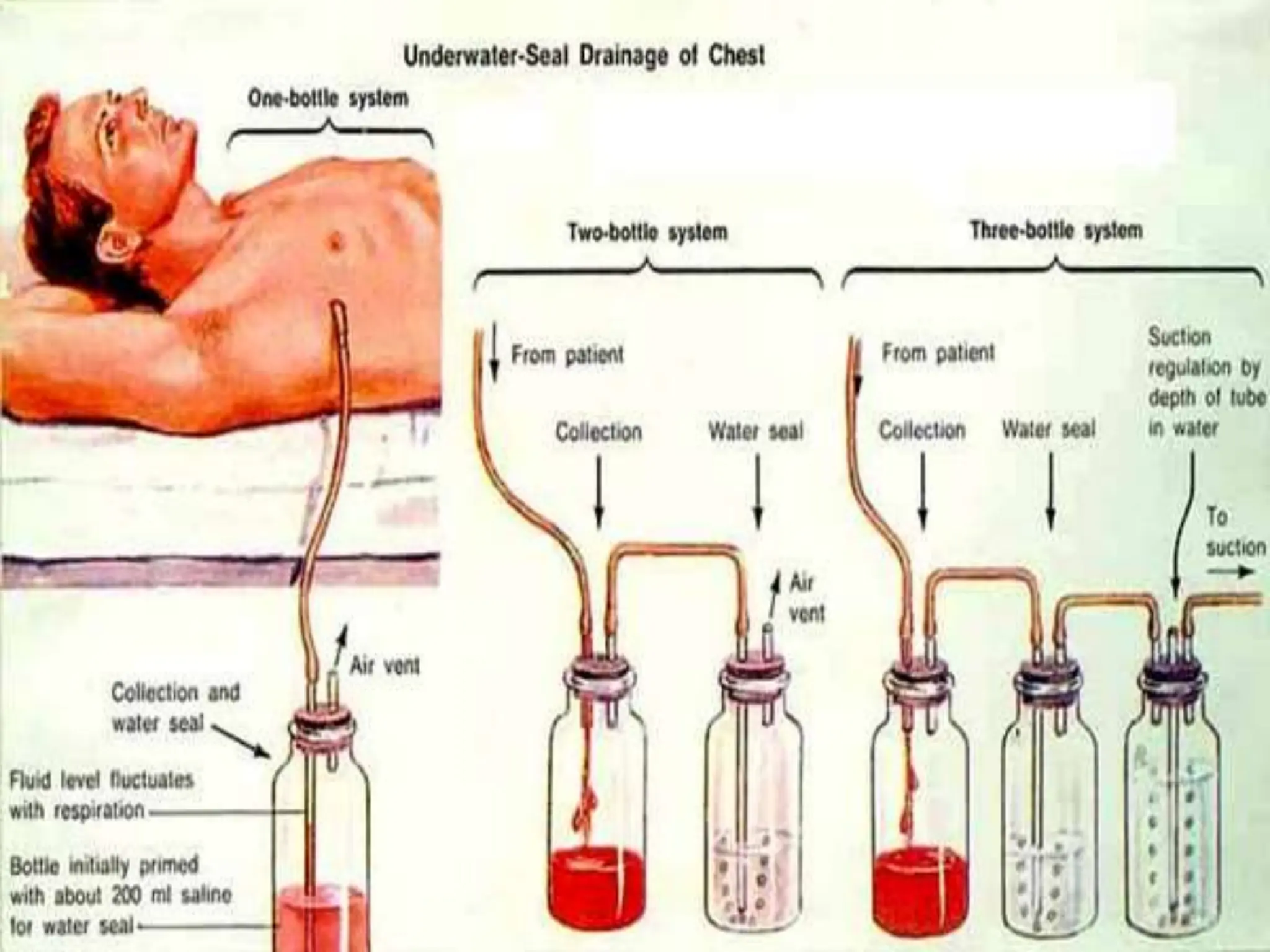
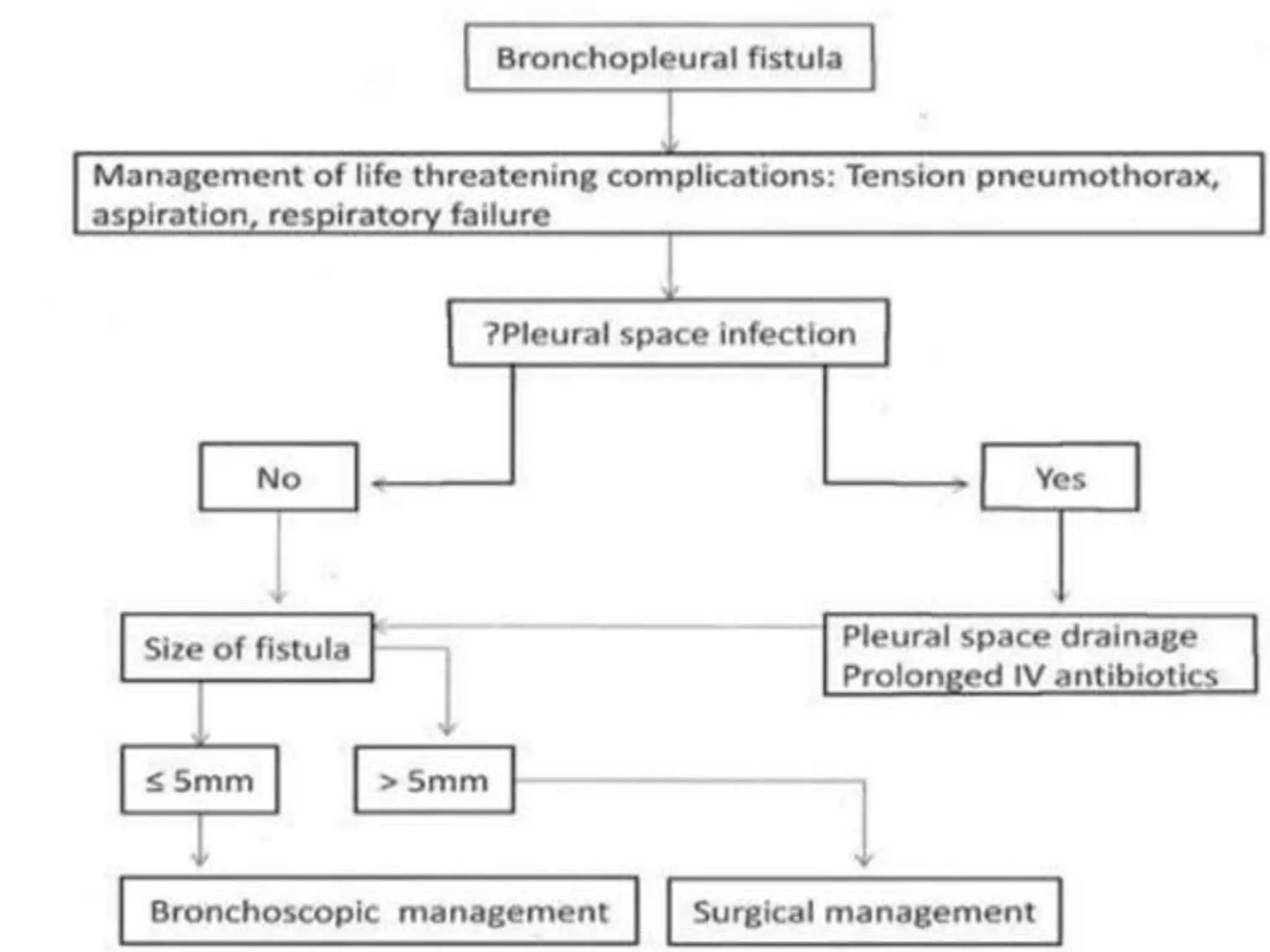
A 15-year-old male was brought to the emergency department 19 days after sustaining a chest injury from a tractor steering wheel. He had pain and breathlessness after the injury and was found to have a near complete transaction of the right main bronchus with bronchopleural fistula (BPF). On examination, he had absent breath sounds on the right side and a chest tube draining fluid. A CT scan showed a right pneumothorax with collapsed lung. BPFs can be classified based on their airflow patterns and location. Treatment depends on the size and chronicity of the fistula and includes medications, endobronchial techniques, surgery, or a combination. The goal of anesthesia management is to optimize