Downloaded 300 times
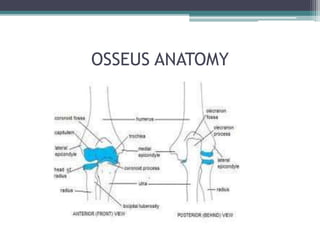
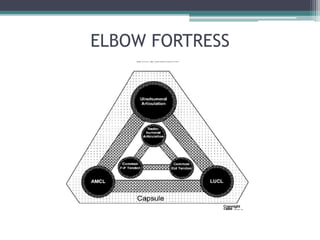
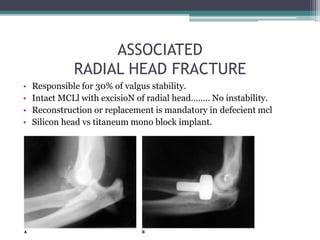


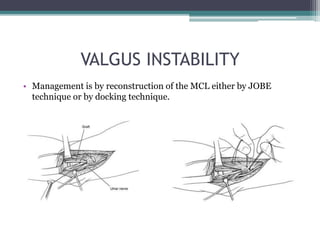

This document discusses elbow instability, including anatomy, stabilizing factors, classification, diagnosis, and management. It covers the soft tissue and bony anatomy of the elbow. Elbow stability relies primarily on the ulnohumeral joint, medial and lateral collateral ligaments. Injuries can range from subluxation to complete dislocation. Diagnosis involves clinical examination and imaging. Management depends on the injury, and may include repair, reconstruction, or fixation of bony and ligamentous injuries.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)










